You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Oracle TuningDocument16 pagesOracle TuningSriram Balasubramanian100% (1)
- Awareness and Practices Among The Selected Senior High School Students About Imposing The First Aid in San Isidro National High SchoolDocument20 pagesAwareness and Practices Among The Selected Senior High School Students About Imposing The First Aid in San Isidro National High SchoolAeido Rosaceae60% (5)
- Pharmacy Facilities RequirementDocument55 pagesPharmacy Facilities RequirementAlex ChinNo ratings yet
- Reviewer: Accounting For Manufacturing OperationsDocument16 pagesReviewer: Accounting For Manufacturing Operationsgab mNo ratings yet
- Chapter-4 Turbine Regulatory Characteristics and Hydraulic TransientsDocument20 pagesChapter-4 Turbine Regulatory Characteristics and Hydraulic TransientsSasankNo ratings yet
- Microbiology Sessions Project IfmsaDocument8 pagesMicrobiology Sessions Project IfmsaRundNo ratings yet
- Autism Final PDFDocument29 pagesAutism Final PDFRundNo ratings yet
- First Draft DVT ProphylaxisDocument6 pagesFirst Draft DVT ProphylaxisRundNo ratings yet
- Water Resources and Management in IraqDocument45 pagesWater Resources and Management in IraqRundNo ratings yet
- Pain Management TherapeuticsDocument10 pagesPain Management TherapeuticsRundNo ratings yet
- 1) Peripheral BloodDocument21 pages1) Peripheral BloodRundNo ratings yet
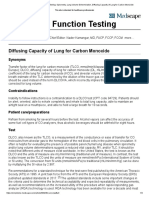
- Pulmonary Function Testing - Spirometry, Lung Volume Determination, Diffusing Capacity of Lung For Carbon MonoxideDocument4 pagesPulmonary Function Testing - Spirometry, Lung Volume Determination, Diffusing Capacity of Lung For Carbon MonoxideRundNo ratings yet
- 3 - Lipids I, II and III PDFDocument60 pages3 - Lipids I, II and III PDFRundNo ratings yet
- Fat EmbolismDocument7 pagesFat EmbolismRundNo ratings yet
- Rund Aljarrah Dana RidaDocument54 pagesRund Aljarrah Dana RidaRundNo ratings yet
- Pediatric SurgeryDocument8 pagesPediatric SurgeryRundNo ratings yet
- Baloglu 2002Document13 pagesBaloglu 2002Marcos VicenteNo ratings yet
- Pan African Enetwork Project Mba Ib: International Institutions and Trade Implications Semester - IiDocument96 pagesPan African Enetwork Project Mba Ib: International Institutions and Trade Implications Semester - IitakangnixonNo ratings yet
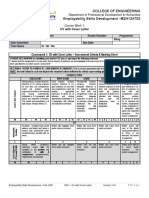
- CW1 - CV With Cover Letter - Assessment Criteria and Marking Sheet - V14.0 - 2Document3 pagesCW1 - CV With Cover Letter - Assessment Criteria and Marking Sheet - V14.0 - 2Malik Mohammed Al SaqriNo ratings yet
- (Official) Unit 7 - Supplementary Materials - PERSPECTIVES 1 (Student Version)Document32 pages(Official) Unit 7 - Supplementary Materials - PERSPECTIVES 1 (Student Version)My BảoNo ratings yet
- Dalija Prasnikar - Delphi Memory ManagmentDocument370 pagesDalija Prasnikar - Delphi Memory ManagmentDenis MartianovNo ratings yet
- Vũ Hoàng Long: Câu HỏiDocument6 pagesVũ Hoàng Long: Câu HỏiĐức TạNo ratings yet
- P2 Day 18 IFRS 15 (Tang) QuestionDocument2 pagesP2 Day 18 IFRS 15 (Tang) QuestionAmanda70% (1)
- Exam3 SolutionDocument6 pagesExam3 Solutionowronrawan74No ratings yet
- Consumer EquilibriumDocument31 pagesConsumer EquilibriumHassanRazaNo ratings yet
- 3.10 Practice Set: Review QuestionsDocument4 pages3.10 Practice Set: Review QuestionsscpNo ratings yet
- Auditing in SchoolsDocument22 pagesAuditing in SchoolsFarahNo ratings yet
- TLE WorksheetDocument9 pagesTLE WorksheetBejiNo ratings yet
- Chapter 22 System Reserved Words BitsDocument29 pagesChapter 22 System Reserved Words BitsRanaIfteeNo ratings yet
- Allama Iqbal Open UniversityDocument2 pagesAllama Iqbal Open UniversityNiamatNo ratings yet
- Notifier 500Document4 pagesNotifier 500Omprakash_jana0% (1)
- ADDRESS1Document12 pagesADDRESS1*IretexNo ratings yet
- I 3031Document222 pagesI 3031Daniel Venancio VieiraNo ratings yet
- Eco Projects Total List From JapanDocument498 pagesEco Projects Total List From JapanJain Sumeet100% (1)
- Activity Design USADocument4 pagesActivity Design USAFredimar CondeNo ratings yet
- FIN425 Intro+Economic Analysis - BariraDocument5 pagesFIN425 Intro+Economic Analysis - BariraBarira NafisaNo ratings yet
- General Instructions (Written Test-Interview)Document7 pagesGeneral Instructions (Written Test-Interview)Umar ButtNo ratings yet
- Mini Baja Lga340Document12 pagesMini Baja Lga340rudey18No ratings yet
- Rojo CCA Self AssessmentDocument3 pagesRojo CCA Self AssessmentRenante DeseoNo ratings yet
- Specifications October 2020 - From 12/ 2020 ProductionDocument13 pagesSpecifications October 2020 - From 12/ 2020 ProductionfraNo ratings yet
- 3.0b INDUSTRIAL SECTORDocument18 pages3.0b INDUSTRIAL SECTORJin Hui TanNo ratings yet