You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Dizziness and VertigoDocument27 pagesDizziness and VertigoPutriAyuWidyastutiRNo ratings yet
- A Homoeopathic Approach To Cancer PDFDocument15 pagesA Homoeopathic Approach To Cancer PDFDishaNo ratings yet
- Ham ADocument1 pageHam Araj1969No ratings yet
- Parenteral Therapy:: Intravenous Therapy (IVT) or VenipunctureDocument3 pagesParenteral Therapy:: Intravenous Therapy (IVT) or VenipunctureMabes100% (1)
- Redefining Wellness: Ultimate Mold GuideDocument11 pagesRedefining Wellness: Ultimate Mold Guidereyshme0% (1)
- Effectiveness of TECAR Therapy and Therapeutic Exercise in The Treatment of Musculoskeletal Conditions A Review ArticleDocument4 pagesEffectiveness of TECAR Therapy and Therapeutic Exercise in The Treatment of Musculoskeletal Conditions A Review ArticleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Introduction To Bio Statistics 2nd Edition R. Sokal F. Rohlf Statistics BiologyDocument190 pagesIntroduction To Bio Statistics 2nd Edition R. Sokal F. Rohlf Statistics BiologyDorilde Tavares100% (4)
- Repertoar Flori de BachDocument74 pagesRepertoar Flori de BachLidia Dicu100% (1)
- Pediatric Assessment ToolDocument3 pagesPediatric Assessment ToolKrystel BatinoNo ratings yet
- Farokh Master Clinical ObservationDocument14 pagesFarokh Master Clinical ObservationDishaNo ratings yet
- Systemic Pathology QuestionDocument4 pagesSystemic Pathology QuestionAnderson Amaro100% (1)
- 05 Paediatrics 25092019Document9 pages05 Paediatrics 25092019DishaNo ratings yet
- Icmr Press Release CovishieldDocument2 pagesIcmr Press Release CovishieldMilanSinghBaisNo ratings yet
- Circular No - 81 - 231120Document2 pagesCircular No - 81 - 231120DishaNo ratings yet
- Serum Institute of India's Fact Sheet For Recipients of Covishield VaccineDocument2 pagesSerum Institute of India's Fact Sheet For Recipients of Covishield VaccineNDTV100% (2)
- OD121984873883813000Document1 pageOD121984873883813000DishaNo ratings yet
- 5 6276139296218939455-1Document603 pages5 6276139296218939455-1Anbreen ShaikNo ratings yet
- Application Process and How To ApplyDocument1 pageApplication Process and How To ApplyDishaNo ratings yet
- Winter-2020 Schedule - 221120Document46 pagesWinter-2020 Schedule - 221120DishaNo ratings yet
- Ethics Basic Concepts ENG PDFDocument76 pagesEthics Basic Concepts ENG PDFJandhyalaNo ratings yet
- A Homoeopathic Case of Alopecia AreataDocument10 pagesA Homoeopathic Case of Alopecia AreataDishaNo ratings yet
- 4144910Document26 pages4144910DishaNo ratings yet
- Synopsis - Adhd - 2Document28 pagesSynopsis - Adhd - 2DishaNo ratings yet
- Changesinadolescents 160704020217 PDFDocument14 pagesChangesinadolescents 160704020217 PDFDishaNo ratings yet
- Project Guidelines For PGD ProgrammmesDocument6 pagesProject Guidelines For PGD ProgrammmesDishaNo ratings yet
- L1 Hypo, Hyperthyroidism and Hashimoto ThyroiditisDocument12 pagesL1 Hypo, Hyperthyroidism and Hashimoto ThyroiditisSivaNo ratings yet
- Seminar DM Bpjs Juni 2014Document28 pagesSeminar DM Bpjs Juni 2014Ari AsriniNo ratings yet
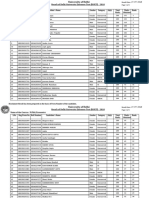
- Name of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Document5 pagesName of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Saiganesh RameshNo ratings yet
- 3descriptive EpidemiologyDocument49 pages3descriptive EpidemiologyAnusha VergheseNo ratings yet
- ADOS 2 Module 4 Revised Algorithm Hus and Lord 2014 April 2022Document2 pagesADOS 2 Module 4 Revised Algorithm Hus and Lord 2014 April 2022DanielNo ratings yet
- Ems NC Iii - SagDocument10 pagesEms NC Iii - SagJaypz DelNo ratings yet
- Extreme Preterm Premature Rupture of Membranes: KSM Obstetri Dan Ginekologi Rumah Sakit Umum Pusat PersahabatanDocument27 pagesExtreme Preterm Premature Rupture of Membranes: KSM Obstetri Dan Ginekologi Rumah Sakit Umum Pusat Persahabatanrilla saeliputriNo ratings yet
- Nursing Management - Colon CancerDocument7 pagesNursing Management - Colon CancerReese Alessandra GandulfoNo ratings yet
- Pain Terms: A Current List With Definitions and Notes On UsageDocument9 pagesPain Terms: A Current List With Definitions and Notes On UsagealexandruNo ratings yet
- Riltrava Aerosphere Epar Product Information enDocument42 pagesRiltrava Aerosphere Epar Product Information enshihyanghuangNo ratings yet
- Fever PresentationDocument15 pagesFever PresentationMaira InaamNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AHector ValleNo ratings yet
- Human Health and DiseaseDocument20 pagesHuman Health and DiseaseA BeheraNo ratings yet
- Hypocalcaemia ESSAYDocument2 pagesHypocalcaemia ESSAYPris AtarashiiNo ratings yet
- ChickenpoxDocument1 pageChickenpoxDavid HylandNo ratings yet
- Graha Roga'sDocument10 pagesGraha Roga'srohinibrajole123No ratings yet
- Chapter 15Document27 pagesChapter 15Jessica nonyeNo ratings yet
- Evaluation and Treatment of Hypertensive Emergencies in AdultsDocument13 pagesEvaluation and Treatment of Hypertensive Emergencies in Adultsjavier ariasNo ratings yet
- Drug Bulletin: Antipsychotic MonitoringDocument4 pagesDrug Bulletin: Antipsychotic MonitoringMuhammad NaufalNo ratings yet
- Allergic Contact Polietileno en El SolarazeDocument16 pagesAllergic Contact Polietileno en El SolarazeFreddy RojasNo ratings yet
- Awake Prone Positioning For Non-Intubated Oxygen Dependent COVID-19 Pneumonia PatientsDocument4 pagesAwake Prone Positioning For Non-Intubated Oxygen Dependent COVID-19 Pneumonia PatientsMuri MurdianaNo ratings yet
- Presentation 1Document18 pagesPresentation 1Talha Mughal Talha MughalNo ratings yet
- Revathi Papsmear ProcedureDocument50 pagesRevathi Papsmear ProcedureRevathi DadamNo ratings yet
- Medicolegal DeathDocument13 pagesMedicolegal DeathWASIF ISMAILNo ratings yet