You might also like
- Claw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandClaw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (1)
- Principles and Management of Acute Orthopaedic Trauma: Third EditionFrom EverandPrinciples and Management of Acute Orthopaedic Trauma: Third EditionNo ratings yet
- Hand PDFDocument179 pagesHand PDFRadenSiwi Bagus HadhiningratNo ratings yet
- Tendon Injuries of Hand: DR Saumya AgarwalDocument101 pagesTendon Injuries of Hand: DR Saumya AgarwaltesfahuntekletilahunNo ratings yet
- Clinical Exam of Hand and Wrist: Guide to Musculoskeletal AssessmentDocument91 pagesClinical Exam of Hand and Wrist: Guide to Musculoskeletal AssessmentjothiNo ratings yet
- De Quervain's Tenosynovitis: Dr. Jatin JR3 Year Orthopaed Ics Fmhs Under SGT UniversityDocument31 pagesDe Quervain's Tenosynovitis: Dr. Jatin JR3 Year Orthopaed Ics Fmhs Under SGT UniversityKuldeep PindariaNo ratings yet
- HIP JOINT Special Tests-WPS OfficeDocument51 pagesHIP JOINT Special Tests-WPS OfficeManisha MishraNo ratings yet
- Kamars RadiologyDocument135 pagesKamars RadiologyNayantara Nair100% (1)
- AO Trauma Vol.2Document100 pagesAO Trauma Vol.2Cujba GheorgheNo ratings yet
- Blue Boxes Upper ArmDocument3 pagesBlue Boxes Upper ArmLardel CarayNo ratings yet
- Any PDFDocument252 pagesAny PDFRaja VeerappanNo ratings yet
- Orthopedic: Dislocations of The Hip JointDocument16 pagesOrthopedic: Dislocations of The Hip JointAnmarNo ratings yet
- Acute Distal Radioulnar Joint InstabilityDocument13 pagesAcute Distal Radioulnar Joint Instabilityyerson fernando tarazona tolozaNo ratings yet
- Orthopedic InjuriesDocument27 pagesOrthopedic InjuriesvikramNo ratings yet
- CTEVDocument25 pagesCTEVIceBearNo ratings yet
- Ankle Anatomy and Blood Supply of TalusDocument66 pagesAnkle Anatomy and Blood Supply of TalusShashank29 LakkalaNo ratings yet
- Gamma NailDocument49 pagesGamma NailMihaela HerghelegiuNo ratings yet
- Peripheral Nerve Disorders: Grades of Injury and Treatment OptionsDocument75 pagesPeripheral Nerve Disorders: Grades of Injury and Treatment OptionsAllahbesertkitaNo ratings yet
- Arm:Leg Fracture PDFDocument11 pagesArm:Leg Fracture PDFHannaNo ratings yet
- Trochanteric #Document20 pagesTrochanteric #Prakash AyyaduraiNo ratings yet
- Forearm fractures and wrist injuriesDocument1 pageForearm fractures and wrist injuriesintan rosliNo ratings yet
- Management of Fractures - DR Matthew SherlockDocument142 pagesManagement of Fractures - DR Matthew Sherlockreeves_cool100% (1)
- External Fixation Principles and Applications.5Document8 pagesExternal Fixation Principles and Applications.5Leonardo Rocha100% (1)
- Gpe - 017.1 - Orthopaedic ExaminationDocument3 pagesGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumNo ratings yet
- Achilles Tendon RuptureDocument19 pagesAchilles Tendon Ruptureapi-509245925No ratings yet
- UKA: When Would I Do It?Document35 pagesUKA: When Would I Do It?neareastspineNo ratings yet
- Avascular Necrosis of The Fibular SesamoidDocument7 pagesAvascular Necrosis of The Fibular SesamoidAlex Yvan Escobedo HinostrozaNo ratings yet
- Chapter 6b Digital SurgeryDocument18 pagesChapter 6b Digital SurgerypodmmgfNo ratings yet
- ZOO3731 chptr.6-8Document55 pagesZOO3731 chptr.6-8Raylax2sik24No ratings yet
- Spine TraumaDocument7 pagesSpine TraumafadlinNo ratings yet
- Osteotomias PediatriaDocument13 pagesOsteotomias PediatriaM Ram CrraNo ratings yet
- Anatomy MS WristJointSGDDocument24 pagesAnatomy MS WristJointSGDSpencerNo ratings yet
- All Papers Topic WiseDocument55 pagesAll Papers Topic WiseZ TariqNo ratings yet
- Ficat and Arlet staging of hip AVNDocument6 pagesFicat and Arlet staging of hip AVNFernando Sugiarto0% (1)
- Distal Humeral Fractures-Current Concepts PDFDocument11 pagesDistal Humeral Fractures-Current Concepts PDFRina AlvionitaNo ratings yet
- Distal Femur Fractures Fixation by Locking Compression Plate-Assessment of Outcome by Rasmussens Functional Knee ScoreDocument7 pagesDistal Femur Fractures Fixation by Locking Compression Plate-Assessment of Outcome by Rasmussens Functional Knee ScoreIJAR JOURNALNo ratings yet
- Ligamentous Injuries About The Ankle and Subtalar Joints: Hans Zwipp, MD, PHD, Stefan Rammelt, MD, Rene Grass, MDDocument35 pagesLigamentous Injuries About The Ankle and Subtalar Joints: Hans Zwipp, MD, PHD, Stefan Rammelt, MD, Rene Grass, MDAnonymous kdBDppigENo ratings yet
- ANATOMY AND BIOMECHANICS OF WRIST JOINT FinalDocument43 pagesANATOMY AND BIOMECHANICS OF WRIST JOINT Finalinas ismailNo ratings yet
- Ankle ComplexDocument95 pagesAnkle ComplexMangala Prema MohanarangamNo ratings yet
- How To Examine The Wrist and HandDocument7 pagesHow To Examine The Wrist and HandSurgicalgownNo ratings yet
- Distal Femur (Sandeep Sir)Document22 pagesDistal Femur (Sandeep Sir)Kirubakaran Saraswathy PattabiramanNo ratings yet
- Flexor Tendon Surgery - 25 Years of Progress - Strickland - JHS 2000Document22 pagesFlexor Tendon Surgery - 25 Years of Progress - Strickland - JHS 2000Professeur Christian DumontierNo ratings yet
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- 22-Surface Anatomy of The Upper and Lower LimbsDocument24 pages22-Surface Anatomy of The Upper and Lower LimbsMiahz Tv100% (1)
- Charnley Ankle ArthrodesisDocument12 pagesCharnley Ankle Arthrodesisdr_s_ganeshNo ratings yet
- Trauma Musculoskeletal - Spine FKK UMJ1Document92 pagesTrauma Musculoskeletal - Spine FKK UMJ1Hendra Hash AwoNo ratings yet
- Crozer-Keystone Ex Tern Ship ManualDocument187 pagesCrozer-Keystone Ex Tern Ship ManualRihamary CruzNo ratings yet
- Treatment of SLAC-CartagenaDocument40 pagesTreatment of SLAC-CartagenaProfesseur Christian DumontierNo ratings yet
- Modified French OsteotomyDocument5 pagesModified French OsteotomyKaustubh KeskarNo ratings yet
- Ministry of Defence Synopsis of Causation Pes PlanusDocument14 pagesMinistry of Defence Synopsis of Causation Pes PlanusSari HestiyariniNo ratings yet
- I. X-Ray Image: Hindfoot Fractures By: Jeremy Tan and Sarah HillDocument8 pagesI. X-Ray Image: Hindfoot Fractures By: Jeremy Tan and Sarah HillSheril MarekNo ratings yet
- B 756 Vertebris GB III10Document44 pagesB 756 Vertebris GB III10Lukasz Bartochowski100% (1)
- Tendon TransferDocument1 pageTendon TransferPandi Smart VjNo ratings yet
- Upper Extremity FracturesDocument80 pagesUpper Extremity FracturesSidan EmozieNo ratings yet
- Biomechanics BHIP JOINTDocument68 pagesBiomechanics BHIP JOINTLinmayee SamalNo ratings yet
- September2010 Clinical GuidelinesDocument26 pagesSeptember2010 Clinical GuidelinesFabianinhoLacerdaNo ratings yet
- Ankle Stability and MovementDocument40 pagesAnkle Stability and MovementBogdan GeangosNo ratings yet
- Hip and Thigh Bones Study QuestionsDocument9 pagesHip and Thigh Bones Study Questionspudding35No ratings yet
- Giant Cell TumorDocument22 pagesGiant Cell TumorMaxmillian Alexander KawilarangNo ratings yet
- DRUJinstabilityreview - PDF 034407Document15 pagesDRUJinstabilityreview - PDF 034407Oscar Cayetano Herrera RodríguezNo ratings yet
- My StomachDocument24 pagesMy StomachPriya GKNo ratings yet
- My PancreasDocument12 pagesMy PancreasPriya GKNo ratings yet
- Case Based Discussion 2-Adjustment Disorder Year 5 Rotation 5Document26 pagesCase Based Discussion 2-Adjustment Disorder Year 5 Rotation 5Priya GKNo ratings yet
- Anatomy of the Large IntestineDocument16 pagesAnatomy of the Large IntestinePriya GKNo ratings yet
- My Basal GangliaDocument18 pagesMy Basal GangliaPriya GKNo ratings yet
- Rectum & Anal Canal AnatomyDocument21 pagesRectum & Anal Canal AnatomyPriya GKNo ratings yet
- Feedback Form WpsDocument2 pagesFeedback Form WpsPriya GKNo ratings yet
- R3 G1 Time TableDocument10 pagesR3 G1 Time TablePriya GKNo ratings yet
- Bell'S Palsy: Ferry Damarjata 20 MARCH 2020Document9 pagesBell'S Palsy: Ferry Damarjata 20 MARCH 2020Priya GKNo ratings yet
- Manage Chronic Kidney Injury in ChildrenDocument29 pagesManage Chronic Kidney Injury in ChildrenPriya GKNo ratings yet
- PsoriasisDocument54 pagesPsoriasisPriya GKNo ratings yet
- Liver TumorsDocument9 pagesLiver TumorsPriya GKNo ratings yet
- Feedback Form WpsDocument2 pagesFeedback Form WpsPriya GKNo ratings yet
- Liver TumorsDocument51 pagesLiver TumorsPriya GKNo ratings yet
- Medicine TT - Yr5-Batch 7 Rot-1, Gp-1Document10 pagesMedicine TT - Yr5-Batch 7 Rot-1, Gp-1Priya GKNo ratings yet
- Feedback Form WpsDocument2 pagesFeedback Form WpsPriya GKNo ratings yet
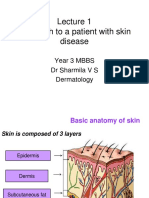
- Approach To Skin DiseasesDocument63 pagesApproach To Skin DiseasesPriya GKNo ratings yet
- Medicine TT - Yr5-Batch 7 Rot-1, Gp-1Document10 pagesMedicine TT - Yr5-Batch 7 Rot-1, Gp-1Priya GKNo ratings yet
- Can You Distinguish Neutral, Formal and Informal Among The Following Groups of WordsDocument3 pagesCan You Distinguish Neutral, Formal and Informal Among The Following Groups of WordsВікторія РудаNo ratings yet
- Hydraulic Oil Hy-Gard Transmission John DeereDocument7 pagesHydraulic Oil Hy-Gard Transmission John DeereLuis Sanchez LlicoNo ratings yet
- English Hand Out for Class 3Document19 pagesEnglish Hand Out for Class 3Pat WibawaNo ratings yet
- Removal of A Pinned Spiral by Generating Target Waves With A Localized StimulusDocument5 pagesRemoval of A Pinned Spiral by Generating Target Waves With A Localized StimulusGretymjNo ratings yet
- Chapter 1 F&B ManagementDocument59 pagesChapter 1 F&B ManagementMohd Faizal Bin AyobNo ratings yet
- UntitledDocument10 pagesUntitledVeneta GizdakovaNo ratings yet
- Brochure HMS LIME 12-04-22 V21Document14 pagesBrochure HMS LIME 12-04-22 V21i10 Sport PlusNo ratings yet
- Goat anatomy and physiology guideDocument8 pagesGoat anatomy and physiology guideLochi GmNo ratings yet
- General Catalogue 2019: UNIOR D.DDocument401 pagesGeneral Catalogue 2019: UNIOR D.DjinpoeNo ratings yet
- BurgerKing Versus McDonaldsDocument4 pagesBurgerKing Versus McDonaldsmarkus johannessenNo ratings yet
- Cerebrospinal Fluid Penetration of Amikacin in Children With Community-Acquired Bacterial MeningitisDocument3 pagesCerebrospinal Fluid Penetration of Amikacin in Children With Community-Acquired Bacterial MeningitisDanny JacobusNo ratings yet
- Pharmacoepidemiology and Environmental HealthDocument3 pagesPharmacoepidemiology and Environmental HealthAashish BhattaraiNo ratings yet
- Adime Malnutrition and OncolgyDocument6 pagesAdime Malnutrition and Oncolgyapi-300587226100% (1)
- Measuring Blood Pressure AccuratelyDocument2 pagesMeasuring Blood Pressure AccuratelyxmantestNo ratings yet
- Manual Instlacion y Servicio Logix Magnum IT and CV ValvesDocument69 pagesManual Instlacion y Servicio Logix Magnum IT and CV ValvesmortifileNo ratings yet
- SGS-GIS-RFC - Combined Version-A4 - v8 - Mar 16 2018Document3 pagesSGS-GIS-RFC - Combined Version-A4 - v8 - Mar 16 2018Refresh CornerNo ratings yet
- De Thi Thu Vao 10 Mon Tieng Anh Quan Dong Da Ha NoiDocument5 pagesDe Thi Thu Vao 10 Mon Tieng Anh Quan Dong Da Ha NoiTrang VuongNo ratings yet
- Atty. Carla Santamaria-Seña Wills and Succession ReviewDocument111 pagesAtty. Carla Santamaria-Seña Wills and Succession ReviewvickimabelliNo ratings yet
- Gym Membership AgreementDocument3 pagesGym Membership Agreementzde thai100% (1)
- ACKSDocument4 pagesACKSPinky Bhattacharyya50% (2)
- PNLE III For Care of Clients With Physiologic and Psychosocial AlterationsDocument10 pagesPNLE III For Care of Clients With Physiologic and Psychosocial AlterationsANGELINE PALATINO100% (1)
- Format No. 1-2019-PSS-01 Rev.1Document1 pageFormat No. 1-2019-PSS-01 Rev.1nithinNo ratings yet
- ACCOMPLISHMENT REPORT School Managed Canteen and WINsDocument7 pagesACCOMPLISHMENT REPORT School Managed Canteen and WINsJohnson Daquiaog BenitezNo ratings yet
- Cranes & Hoists ProgramDocument28 pagesCranes & Hoists ProgramImtiyaz AkhtarNo ratings yet
- بﻮﺤﻟا ﻦﺤﻃ ﺔﻧﺎﻘﺗ - Cereal Milling Technology: · January 2013Document202 pagesبﻮﺤﻟا ﻦﺤﻃ ﺔﻧﺎﻘﺗ - Cereal Milling Technology: · January 2013Moh Al Basher BabikerNo ratings yet
- Diagnostic Test Science 5Document7 pagesDiagnostic Test Science 5Rex Russel SalemNo ratings yet
- 1st SemesterDocument28 pages1st SemesterSathiya SarangapaniNo ratings yet
- PDF Fcuk CTLG 2020 Split 01Document46 pagesPDF Fcuk CTLG 2020 Split 01Ted Andrew AbalosNo ratings yet
- CIE IGCSE BiologyDocument25 pagesCIE IGCSE Biologytgdzbspikio.comNo ratings yet
- August 2016Document15 pagesAugust 2016Pumper Trader0% (1)