You might also like
- Prostate: Saeed AliDocument56 pagesProstate: Saeed Alisaeedali84842461No ratings yet
- Mri of Prostate and Endorectal Mri Final1Document70 pagesMri of Prostate and Endorectal Mri Final1Sunny SbaNo ratings yet
- Prostate and Seminal VesiclesDocument83 pagesProstate and Seminal Vesiclesgreg_enricoNo ratings yet
- Prostate GlandDocument54 pagesProstate Glanddr_shamimrNo ratings yet
- Trus Biopsy RohanDocument61 pagesTrus Biopsy RohanRohan BatraNo ratings yet
- Urinary Tract TumourDocument40 pagesUrinary Tract TumourNu JoeNo ratings yet
- Prostate Cancer Imaging July, 2020 - ICI 01Document42 pagesProstate Cancer Imaging July, 2020 - ICI 01madvincyNo ratings yet
- DI Abdomen P 674 737 PART 2 SEC 3Document64 pagesDI Abdomen P 674 737 PART 2 SEC 3tudoranluciana1No ratings yet
- EAU Pocket On Primary Urethral Carcinoma 2022Document9 pagesEAU Pocket On Primary Urethral Carcinoma 2022AlbalushiNo ratings yet
- Renal Cell CarcinomaDocument10 pagesRenal Cell Carcinoma'asyura Mohd RezaNo ratings yet
- URORADIOLOGYDocument34 pagesURORADIOLOGYMeg AmoonNo ratings yet
- Finalcaprostate 180114163813 PDFDocument124 pagesFinalcaprostate 180114163813 PDFAlchemi ANo ratings yet
- Benign Prostatic Hyperplasia: Pembimbing: DR Herinto Himawan Sp.UDocument42 pagesBenign Prostatic Hyperplasia: Pembimbing: DR Herinto Himawan Sp.Uilma aulia zahraNo ratings yet
- Carcinoma Rectum - Janak - NEWDocument74 pagesCarcinoma Rectum - Janak - NEWTowhidulIslamNo ratings yet
- CarcinomarectumDocument45 pagesCarcinomarectumHuzefa MemonNo ratings yet
- Prostatic Hyperplasia: Terminology Top Differential DiagnosesDocument1 pageProstatic Hyperplasia: Terminology Top Differential DiagnosesMilton Kaspo Sagoya IIINo ratings yet
- Disorders of The Prostate: Dr.M.Galuh Richata, SpuDocument32 pagesDisorders of The Prostate: Dr.M.Galuh Richata, SpuEmallia Phypiet FitrianiNo ratings yet
- Cancer ProstateDocument4 pagesCancer ProstateOkki Masitah Syahfitri NasutionNo ratings yet
- Ecografía ProstaticaDocument9 pagesEcografía ProstaticadynachNo ratings yet
- BPHDocument25 pagesBPHsurya mertayasaNo ratings yet
- Small Bowel LymphomaDocument30 pagesSmall Bowel LymphomaeosfieldNo ratings yet
- Neoplasms of The Genitourinary TractDocument71 pagesNeoplasms of The Genitourinary Tractvishalzenia100% (2)
- Benign Prostatic HyperplasiaDocument34 pagesBenign Prostatic Hyperplasiaanwar jabariNo ratings yet
- A Case of Retrorectal MassDocument33 pagesA Case of Retrorectal MassPrasanth NarayananNo ratings yet
- Salivary TumorDocument54 pagesSalivary TumorPartha GanesanNo ratings yet
- 11 Prostate CancerDocument52 pages11 Prostate Cancerclaire yowsNo ratings yet
- MS, Frcs (England), Frcs (Edinburgh), Frcs (Glasgow)Document52 pagesMS, Frcs (England), Frcs (Edinburgh), Frcs (Glasgow)Anis HospitalNo ratings yet
- Benign Prostate HyperplasiaDocument49 pagesBenign Prostate HyperplasiaRohani TaminNo ratings yet
- Radiologi Onkologi: Muhammad Iqbal Dr. Rony Rustam, SPB (K) OnkDocument8 pagesRadiologi Onkologi: Muhammad Iqbal Dr. Rony Rustam, SPB (K) OnkakreditasirsurNo ratings yet
- Radiologi EndokrinDocument76 pagesRadiologi EndokrinAndi9993100% (1)
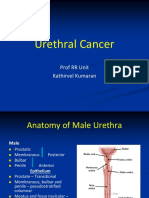
- Urethral CancersDocument24 pagesUrethral CancersKousik AmancharlaNo ratings yet
- Kuliah Prostat (2) RevisiDocument32 pagesKuliah Prostat (2) RevisiAditya PrambudhiNo ratings yet
- Kuliah Blok Neoplasma - Januari 2011 - 2Document161 pagesKuliah Blok Neoplasma - Januari 2011 - 2Natallia BatuwaelNo ratings yet
- Kuliah Blok Neoplasma - Januari 2011Document161 pagesKuliah Blok Neoplasma - Januari 2011Natallia BatuwaelNo ratings yet
- Soft Tissue Sarcomas ofDocument35 pagesSoft Tissue Sarcomas ofmogesie1995No ratings yet
- Urology Lecture No. 4 - Urological CancersDocument71 pagesUrology Lecture No. 4 - Urological CancersLantoş Filip FernandoNo ratings yet
- Adjuvant Pancreas (Post-Op) AtlasDocument31 pagesAdjuvant Pancreas (Post-Op) AtlasDetelina Walchewa-Nedewa100% (1)
- MX Protocols Oropharyngeal Malignancy CompatDocument42 pagesMX Protocols Oropharyngeal Malignancy CompatBikram ChoudhuryNo ratings yet
- Urinary Tract CancerDocument53 pagesUrinary Tract CancerandikaisnaeniNo ratings yet
- A2 Prostate Ca - AinDocument4 pagesA2 Prostate Ca - AinNur Liyana Ahmad ZakiNo ratings yet
- TP Thyroid Nodules 1Document59 pagesTP Thyroid Nodules 1Meaw Thitirat SupasilNo ratings yet
- Marion Swall, MIV USC School of MedicineDocument18 pagesMarion Swall, MIV USC School of MedicineAnonymous rna2NXPc9QNo ratings yet
- Prostate GlandDocument14 pagesProstate GlandJake MillerNo ratings yet
- Renal NeoplasmDocument153 pagesRenal NeoplasmTHESSNAVARRO100% (2)
- Lecture09 Radiological Examination of The Liver, Biliary Tract and PancreasDocument56 pagesLecture09 Radiological Examination of The Liver, Biliary Tract and PancreassinisarNo ratings yet
- Marion Swall, MIV USC School of MedicineDocument18 pagesMarion Swall, MIV USC School of Medicinemynoidanh19No ratings yet
- Prostate Cancer 1Document39 pagesProstate Cancer 1Rohaan Imtiaz 2No ratings yet
- Parapharyngeal Space TumorsDocument60 pagesParapharyngeal Space TumorsHossam ThabetNo ratings yet
- EAU Pocket On Renal Cell Carcinoma 2022Document28 pagesEAU Pocket On Renal Cell Carcinoma 2022Dane QhNo ratings yet
- Manov 2020Document8 pagesManov 2020kanaNo ratings yet
- Surgical RX of Cancer 2023 - BNS 313Document32 pagesSurgical RX of Cancer 2023 - BNS 313Kemo RakhoboNo ratings yet
- MR Af ProstataDocument8 pagesMR Af ProstataKamran AfzalNo ratings yet
- Bab I, II Season 2Document21 pagesBab I, II Season 2Mu'thia MustaqimNo ratings yet
- Prostate Ca PathologyDocument7 pagesProstate Ca Pathologymaria andreasNo ratings yet
- Computed Tomography of The Prostate-A Review: J GossnerDocument8 pagesComputed Tomography of The Prostate-A Review: J GossnerFdr. MurniNo ratings yet
- Prostate CancerDocument10 pagesProstate Canceraji20No ratings yet
- Cancer of PancreasDocument50 pagesCancer of PancreasIsaac MwangiNo ratings yet
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- Contrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsFrom EverandContrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsWen-Ping WangNo ratings yet
- Brachial Plexus Injury LatestDocument37 pagesBrachial Plexus Injury LatestRajhmuniran KandasamyNo ratings yet
- Approach To Common Respiratory DiseaseDocument57 pagesApproach To Common Respiratory DiseaseRajhmuniran KandasamyNo ratings yet
- Examination Of: ThyroidDocument49 pagesExamination Of: ThyroidRajhmuniran KandasamyNo ratings yet
- Per Rectal Bleeding CompiledDocument33 pagesPer Rectal Bleeding CompiledRajhmuniran Kandasamy100% (1)
- Investigations For Pcos: Rajhmuniran KandasamyDocument21 pagesInvestigations For Pcos: Rajhmuniran KandasamyRajhmuniran KandasamyNo ratings yet
- Natural History AND Classification FibroidDocument8 pagesNatural History AND Classification FibroidRajhmuniran KandasamyNo ratings yet
- Paed Condition & Gait SeminarDocument18 pagesPaed Condition & Gait SeminarRajhmuniran KandasamyNo ratings yet
- Seminar 3 ImmunizationDocument42 pagesSeminar 3 ImmunizationRajhmuniran KandasamyNo ratings yet
- Nasal Discharge & ObstructionDocument70 pagesNasal Discharge & ObstructionRajhmuniran KandasamyNo ratings yet
- Oncology CasesDocument96 pagesOncology CasesPrutha Vaidya100% (1)
- Exploring Medical Language 10th Brooks Test BankDocument16 pagesExploring Medical Language 10th Brooks Test BankRaadqqqNo ratings yet
- Radiologic Management of Thoracic Nodules and MassesDocument14 pagesRadiologic Management of Thoracic Nodules and MassesVianney OlveraNo ratings yet
- 1.understanding Cancer PPT LectureDocument184 pages1.understanding Cancer PPT LectureCherry Lou GuanzingNo ratings yet
- Neutrophils in Pancreatic Cancer ProgressionDocument103 pagesNeutrophils in Pancreatic Cancer ProgressionShahid ShaikhNo ratings yet
- Case Study Breast CancerDocument25 pagesCase Study Breast CancerRalph Neil Manlutac100% (1)
- Cancer NotesDocument6 pagesCancer NotesRocco WalksNo ratings yet
- 138 FullDocument6 pages138 Fullamor letrasNo ratings yet
- Rickettsia, Mycoplasma. Fungi, ProtozoaDocument4 pagesRickettsia, Mycoplasma. Fungi, ProtozoaVincent ReyesNo ratings yet
- CancerDocument19 pagesCancerShehada Marcos BondadNo ratings yet
- ACR In-Service 2007 Exam, Answers, RationalDocument98 pagesACR In-Service 2007 Exam, Answers, RationalDave FullerNo ratings yet
- Use of CoQ10 To Treat MalignanciesDocument2 pagesUse of CoQ10 To Treat MalignanciesTUartistNo ratings yet
- Prof. Marco GiammancoDocument159 pagesProf. Marco GiammancomarcogiammancoNo ratings yet
- 6 Hos CarcinogenesisDocument90 pages6 Hos CarcinogenesisalgutNo ratings yet
- NutrientsDocument14 pagesNutrientsSteve GannabanNo ratings yet
- 2239-Article Text-3613-1-10-20200304Document4 pages2239-Article Text-3613-1-10-20200304Abdul HakeemNo ratings yet
- Microscopic Slides Pathology-2Document135 pagesMicroscopic Slides Pathology-2Justin JannatiNo ratings yet
- Past Papers 1 200Document55 pagesPast Papers 1 200AmarAldujaili100% (1)
- Treating Gallbladder Cancer - A Quick GuideDocument9 pagesTreating Gallbladder Cancer - A Quick GuideSpongebob57No ratings yet
- Giant Cell Tumor - CompleteDocument35 pagesGiant Cell Tumor - CompletewildanmalikNo ratings yet
- PosterDocument45 pagesPosterRoxana Alexandra BogosNo ratings yet
- Driving Menarini's Future With Decisive Steps - ScripDocument4 pagesDriving Menarini's Future With Decisive Steps - ScripJins100% (1)
- Breast and Lung CancerDocument141 pagesBreast and Lung CancerabdurehmanNo ratings yet
- Cancer de PancreasDocument12 pagesCancer de PancreasRuben RoaNo ratings yet
- Ewing's Sarcoma Case StudyDocument24 pagesEwing's Sarcoma Case StudyMary Justine Nuyad-Africa100% (1)
- AngiogenezaDocument19 pagesAngiogenezaamaliaanghelNo ratings yet
- 1 s2.0 S0092867422011734 MainDocument29 pages1 s2.0 S0092867422011734 MainIoanna NikdimaNo ratings yet
- Uterine Smooth Muscle Tumors of Unknown Malignant Potential - A Challenging QuestionDocument7 pagesUterine Smooth Muscle Tumors of Unknown Malignant Potential - A Challenging QuestionArt AdibahNo ratings yet
- NLS DiagnosticsDocument71 pagesNLS DiagnosticsMarkus van der WesthuizenNo ratings yet
- Signs and SymptomsDocument8 pagesSigns and SymptomsGehla TumananNo ratings yet