You might also like
- FINAL Food Addiction Tool Kit 10-14-15Document59 pagesFINAL Food Addiction Tool Kit 10-14-15Torc Steele100% (1)
- FDARDocument33 pagesFDARRaquel M. Mendoza100% (7)
- Dr. Sourav Chowdhury Senior ResidentDocument79 pagesDr. Sourav Chowdhury Senior ResidentBhawna JoshiNo ratings yet
- Ectopicpregnancy Most ImpDocument79 pagesEctopicpregnancy Most Impﻣﻠﻚ عيسىNo ratings yet
- Ectopic Pregnancy Diagnosis and ManagementDocument44 pagesEctopic Pregnancy Diagnosis and ManagementDegefaw BikoyNo ratings yet
- Ectopic PregnancyDocument34 pagesEctopic Pregnancyannu panchalNo ratings yet
- Diagnosing Ectopic Pregnancy with Beta-hCG and UltrasoundDocument7 pagesDiagnosing Ectopic Pregnancy with Beta-hCG and UltrasoundSe CretNo ratings yet
- Ectopic Pregnancy1Document34 pagesEctopic Pregnancy1Kreshimaricon FurigayNo ratings yet
- Ectopic Pregnancy FocusDocument62 pagesEctopic Pregnancy FocusrajaeasNo ratings yet
- Ectopic Pregnancy: DR .Urmila KarkiDocument27 pagesEctopic Pregnancy: DR .Urmila KarkiBasudev chNo ratings yet
- Ectopic Pregnancy Diagnosis and TreatmentDocument61 pagesEctopic Pregnancy Diagnosis and TreatmentSuchie ILyasNo ratings yet
- Ectopic PregnancyDocument7 pagesEctopic Pregnancymendato marcabanNo ratings yet
- Ectopic PregnancyDocument32 pagesEctopic Pregnancyyt2zkpkphqNo ratings yet
- Ectopic Pregnancy ADocument37 pagesEctopic Pregnancy AJervhen Sky Adolfo Dalisan100% (1)
- Abortion Guide: Causes, Types, Symptoms & TreatmentDocument36 pagesAbortion Guide: Causes, Types, Symptoms & TreatmentdimlyNo ratings yet
- Ectopic Pregnancy: Causes, Symptoms and DiagnosisDocument60 pagesEctopic Pregnancy: Causes, Symptoms and DiagnosisAndrada Doţa100% (1)
- Ectopic PregnancyDocument14 pagesEctopic PregnancytaufiqNo ratings yet
- Ectopic Pregnancy (Autosaved)Document56 pagesEctopic Pregnancy (Autosaved)susmita shresthaNo ratings yet
- Obstetric Emergencies: First - Trimester Pregnancy EmergenciesDocument14 pagesObstetric Emergencies: First - Trimester Pregnancy EmergenciesdianNo ratings yet
- CCD - Ectopic Pregnancy HafyzDocument29 pagesCCD - Ectopic Pregnancy HafyzHanif GandohNo ratings yet
- कर हर मैदान फ़तेह - Abortion का संक्षिप्त विवरणDocument38 pagesकर हर मैदान फ़तेह - Abortion का संक्षिप्त विवरणdimlyNo ratings yet
- EP C2 by EliDocument40 pagesEP C2 by EliElsai EsbNo ratings yet
- Ectopic Pregnancy: Understanding Causes, Symptoms and TreatmentDocument47 pagesEctopic Pregnancy: Understanding Causes, Symptoms and TreatmentMuhammad AbeeshNo ratings yet
- Ectopic Pregnancy Surgical Management, Non Surgical - Syifa ShafiraDocument45 pagesEctopic Pregnancy Surgical Management, Non Surgical - Syifa ShafiraSyifa ShafiraNo ratings yet
- Ectopic Pregnancy Student LectureDocument19 pagesEctopic Pregnancy Student Lectureapi-370504650% (4)
- Etopic PregnancyDocument15 pagesEtopic PregnancyAileenNo ratings yet
- Ectopic Pregnancy BWDocument28 pagesEctopic Pregnancy BWZiya AkhtarNo ratings yet
- Ectopic PregnancyDocument27 pagesEctopic Pregnancyاحمد احمدNo ratings yet
- Ultrasonographic Diagnosis and Management of Ectopic PregnancyDocument25 pagesUltrasonographic Diagnosis and Management of Ectopic PregnancyMuhammad AbeeshNo ratings yet
- Ectopic Pregnancy: Deomicah D. SolanoDocument42 pagesEctopic Pregnancy: Deomicah D. SolanoJann ericka JaoNo ratings yet
- GynecologyDocument18 pagesGynecologyLuai Tuma KhouryNo ratings yet
- Definition: Genital Tract Bleeding From 28th Incidence: 2 - 3 % of All PregnanciesDocument31 pagesDefinition: Genital Tract Bleeding From 28th Incidence: 2 - 3 % of All PregnanciesMRT RadiologyNo ratings yet
- Understanding miscarriage: causes, types, symptoms, and treatmentDocument38 pagesUnderstanding miscarriage: causes, types, symptoms, and treatmentzianab aliNo ratings yet
- Ectopicpregnancy30 10 14 150420090454 Conversion Gate01 PDFDocument104 pagesEctopicpregnancy30 10 14 150420090454 Conversion Gate01 PDFchetankumarbhumireddyNo ratings yet
- Ectopic PregnancyDocument26 pagesEctopic PregnancyMalek.Fakher1900No ratings yet
- Ectopic PregnancyDocument18 pagesEctopic PregnancyWondimu EliasNo ratings yet
- Ectopic Pregnancy: Aldilyn J. Sarajan, MD, MPH 2 Year Ob-Gyn Resident ZCMCDocument61 pagesEctopic Pregnancy: Aldilyn J. Sarajan, MD, MPH 2 Year Ob-Gyn Resident ZCMCDee SarajanNo ratings yet
- Early Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelDocument60 pagesEarly Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelmedicoNo ratings yet
- NCM 107 Skills Lab Results 1Document85 pagesNCM 107 Skills Lab Results 1Joseph DusichNo ratings yet
- Ectopic 2Document48 pagesEctopic 2Norsri WahyuNo ratings yet
- Ectopic Pregnancy Diagnosis and TreatmentDocument25 pagesEctopic Pregnancy Diagnosis and TreatmentIbrahim JameelallaNo ratings yet
- Womens Health For Medical Finals (Based On Newcastle University Learning Outcomes)Document133 pagesWomens Health For Medical Finals (Based On Newcastle University Learning Outcomes)RedTabs100% (2)
- OBS Review Session Suzanne Ectopic PregnancyDocument7 pagesOBS Review Session Suzanne Ectopic PregnancyhitowaNo ratings yet
- Ectopic Pregnancy: Causes, Symptoms and Treatment OptionsDocument2 pagesEctopic Pregnancy: Causes, Symptoms and Treatment OptionsLuis PadillaNo ratings yet
- Ectopic Pregnancy: Causes, Symptoms and Treatment OptionsDocument2 pagesEctopic Pregnancy: Causes, Symptoms and Treatment OptionsKrista P. AguinaldoNo ratings yet
- Culdocentesis: G. Richard Braen and David Lee PierceDocument6 pagesCuldocentesis: G. Richard Braen and David Lee PierceebolynsurivNo ratings yet
- Ectopic Pregnancy5Document39 pagesEctopic Pregnancy5Muhammad AbeeshNo ratings yet
- Maternity 2 Ante-Partum Haemorrhage (Aph) 26.3.2021Document29 pagesMaternity 2 Ante-Partum Haemorrhage (Aph) 26.3.2021Siti Nur Amalia FaizalNo ratings yet
- PREGNANC1Document20 pagesPREGNANC1SriramNo ratings yet
- 25ECTOPICDocument4 pages25ECTOPIChanselMDNo ratings yet
- Approach To Patient With Ovarian Cysts: Done By: Yahyia Al-Abri 90440Document53 pagesApproach To Patient With Ovarian Cysts: Done By: Yahyia Al-Abri 90440NinaNo ratings yet
- Ectopic Pregnancy Diagnosis and TreatmentDocument73 pagesEctopic Pregnancy Diagnosis and TreatmentdeevoncNo ratings yet
- Ectopic Pregnancy GuideDocument4 pagesEctopic Pregnancy GuideIGA ABRAHAMNo ratings yet
- Ectopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentDocument43 pagesEctopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentAlrick AsentistaNo ratings yet
- OBSTETRICS & GYNAECOLOGY GUIDELINESDocument84 pagesOBSTETRICS & GYNAECOLOGY GUIDELINESselvie87100% (2)
- Management of Pregnancy Related BleedingDocument75 pagesManagement of Pregnancy Related BleedingChuah Wei Hong100% (1)
- Ectopic PregnancyDocument3 pagesEctopic PregnancySiska FriedmanNo ratings yet
- Cephalopelvic DisproportionDocument6 pagesCephalopelvic DisproportionBaljinder kaurNo ratings yet
- Molar PregnancyDocument15 pagesMolar Pregnancyapi-3705046No ratings yet
- Lower Genital Tract Precancer: Colposcopy, Pathology and TreatmentFrom EverandLower Genital Tract Precancer: Colposcopy, Pathology and TreatmentNo ratings yet
- Factors Affecting Use of Magnesium Sulphate For Pre-Eclampsia or Eclampsia - A Qualitative Evidence SynthesisDocument13 pagesFactors Affecting Use of Magnesium Sulphate For Pre-Eclampsia or Eclampsia - A Qualitative Evidence Synthesismember12dNo ratings yet
- Steroids, Steroid Associated Substances, and Gestational Diabetes MellitusDocument18 pagesSteroids, Steroid Associated Substances, and Gestational Diabetes Mellitusmember12dNo ratings yet
- Ultrasound Estimated Subcutaneous and Visceral Adipose Tissue Thicknesses and Risk of Pre EclampsiaDocument8 pagesUltrasound Estimated Subcutaneous and Visceral Adipose Tissue Thicknesses and Risk of Pre Eclampsiamember12dNo ratings yet
- Vitamin D Deficiency and Gestational Diabetes Mellitus in Relation To Body Mass IndexDocument10 pagesVitamin D Deficiency and Gestational Diabetes Mellitus in Relation To Body Mass Indexmember12dNo ratings yet
- Dietary Factors That Affect The Risk of Pre-EclampsiaDocument16 pagesDietary Factors That Affect The Risk of Pre-Eclampsiamember12dNo ratings yet
- Pre-Eclampsia Is A Valuable Opportunity To Diagnose Chronic Kidney Disease - A Multicentre StudyDocument11 pagesPre-Eclampsia Is A Valuable Opportunity To Diagnose Chronic Kidney Disease - A Multicentre Studymember12dNo ratings yet
- Physical Activity and The Occurence of Postpartum Depression - A Systematic ReviewDocument25 pagesPhysical Activity and The Occurence of Postpartum Depression - A Systematic Reviewmember12dNo ratings yet
- Ino Gynecology II Outpatient (13 September 2021)Document1 pageIno Gynecology II Outpatient (13 September 2021)member12dNo ratings yet
- Patient Recapitulation Delivery Room ReportDocument2 pagesPatient Recapitulation Delivery Room Reportmember12dNo ratings yet
- Ram Poli Urogin 13.9.21Document1 pageRam Poli Urogin 13.9.21member12dNo ratings yet
- Depression Is A Serious Mental Health ProblemDocument2 pagesDepression Is A Serious Mental Health Problemmember12dNo ratings yet
- Kom-Daily Cot Monday 13.09.21 FixDocument3 pagesKom-Daily Cot Monday 13.09.21 Fixmember12dNo ratings yet
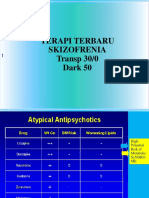
- Terapi Terbaru Skizofrenia Transp 30/0 Dark 50Document58 pagesTerapi Terbaru Skizofrenia Transp 30/0 Dark 50member12dNo ratings yet
- TUGAS CRITICAL APRAISAL - 03 - Abi Rafdi - Obstetri Dan GinekologiDocument4 pagesTUGAS CRITICAL APRAISAL - 03 - Abi Rafdi - Obstetri Dan Ginekologimember12dNo ratings yet
- Mola Hidatidosa JESDocument24 pagesMola Hidatidosa JESmember12dNo ratings yet
- Daftar PustakaDocument1 pageDaftar Pustakamember12dNo ratings yet
- Status Pasien Dengan Keluhan Nyeri BAKDocument5 pagesStatus Pasien Dengan Keluhan Nyeri BAKmember12dNo ratings yet
- Pregnancy Infection Guide: TORCH PathogensDocument59 pagesPregnancy Infection Guide: TORCH Pathogensmember12dNo ratings yet
- One Lung VentilationDocument2 pagesOne Lung Ventilationmember12dNo ratings yet
- Daftar PustakaDocument1 pageDaftar Pustakamember12dNo ratings yet
- One Lung VentilationDocument2 pagesOne Lung Ventilationmember12dNo ratings yet
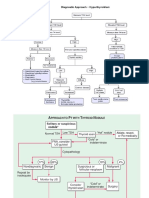
- Diagnostic Approach ThyroidDocument3 pagesDiagnostic Approach Thyroidmember12dNo ratings yet
- Baru Metabolisme LipidDocument14 pagesBaru Metabolisme Lipidmember12dNo ratings yet
- Daftar PustakaDocument1 pageDaftar Pustakamember12dNo ratings yet
- Hospital Pharmacy Article Reviews Pregabalin for Neuropathic PainDocument16 pagesHospital Pharmacy Article Reviews Pregabalin for Neuropathic PainadityaNo ratings yet
- Gordon's 11 Functional Health PatternDocument2 pagesGordon's 11 Functional Health PatternWendell AcuñaNo ratings yet
- NCP FinalDocument4 pagesNCP Finalmarkanthony3903No ratings yet
- Diagnosis and Treatment Planning in Conservative Dentistry and Endodontics / Orthodontic Courses by Indian Dental AcademyDocument44 pagesDiagnosis and Treatment Planning in Conservative Dentistry and Endodontics / Orthodontic Courses by Indian Dental Academyindian dental academy100% (3)
- Kibreet With ImagesDocument260 pagesKibreet With Imagesعباس عبداللهNo ratings yet
- Status EpilepticusDocument22 pagesStatus EpilepticusVivi Kristiani RumapeaNo ratings yet
- Stool Exam Guide - Key Tests, Colors, Consistencies in 40 CharactersDocument8 pagesStool Exam Guide - Key Tests, Colors, Consistencies in 40 CharactersLester John HilarioNo ratings yet
- Contoh SoapDocument11 pagesContoh SoapIlham riandaNo ratings yet
- Food Allergy Concept MapDocument4 pagesFood Allergy Concept MapIzhra MargateNo ratings yet
- Synovial ChondromatosisDocument4 pagesSynovial ChondromatosisNadia Bordaş100% (1)
- Habib 2009Document45 pagesHabib 2009Catherine MorrisNo ratings yet
- SELECTION OF PUBLICATIONS-BACTALERT VIRTUO 9312725 010GBB Web PDFDocument21 pagesSELECTION OF PUBLICATIONS-BACTALERT VIRTUO 9312725 010GBB Web PDFSaifuddin KhaledNo ratings yet
- Risk of Arrhythmia and Sudden Death - M. Malik (BMJ, 2001) WWDocument429 pagesRisk of Arrhythmia and Sudden Death - M. Malik (BMJ, 2001) WWRohan Upadhyay UpadhyayNo ratings yet
- Worksheet 1 (Before Lec 1) PDFDocument4 pagesWorksheet 1 (Before Lec 1) PDFLei Zaira BiendimaNo ratings yet
- GCS dan REMS dalam Memprediksi Outcome Pasien Trauma KepalaDocument12 pagesGCS dan REMS dalam Memprediksi Outcome Pasien Trauma KepalaSatria Yosi HernawanNo ratings yet
- Deep Fungal InfectionsDocument33 pagesDeep Fungal Infectionstummalapalli venkateswara raoNo ratings yet
- Health 9 Q3 M2Document14 pagesHealth 9 Q3 M2Jorely Barbero MundaNo ratings yet
- 5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal OcclusionsDocument5 pages5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal Occlusionsthiên lữNo ratings yet
- Loratadine Drug StudyDocument1 pageLoratadine Drug StudyShene Claire VigillaNo ratings yet
- Approach To Unknown Drug OverdoseDocument3 pagesApproach To Unknown Drug OverdoseRobert So JrNo ratings yet
- Patente Sida...Document9 pagesPatente Sida...VictorVanderFoxysNo ratings yet
- 10.7 The Lymphatic System Extra NotesDocument5 pages10.7 The Lymphatic System Extra NotesVinieysha LoganathanNo ratings yet
- E01 AeromedicalDocument28 pagesE01 AeromedicalRumahorbo Hinsa JulianNo ratings yet
- CT Bowel WallDocument12 pagesCT Bowel WallBrian LucasNo ratings yet
- HematologyDocument6 pagesHematologyRian CopperNo ratings yet
- Fact Sheet on Emerging and Re-Emerging Infectious DiseasesDocument7 pagesFact Sheet on Emerging and Re-Emerging Infectious DiseasesAmanda PratiwiNo ratings yet
- Contoh CJRDocument16 pagesContoh CJRmmerry743No ratings yet
- Mosaicplasty 1030208g UsDocument12 pagesMosaicplasty 1030208g UsAnil SoodNo ratings yet