You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Where There Is No DoctorDocument503 pagesWhere There Is No DoctorDeborah Mertsch100% (14)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Evaluation of The Painful Total Knee Arthroplasty.99377Document9 pagesEvaluation of The Painful Total Knee Arthroplasty.99377Filip starcevic100% (1)
- Personal Development Planning Journal: © The Performance CollectiveDocument22 pagesPersonal Development Planning Journal: © The Performance CollectiveTahir AzizNo ratings yet
- Demonstrate Knowledge of The Stages of Child DevelopmentDocument64 pagesDemonstrate Knowledge of The Stages of Child DevelopmentAvaNo ratings yet
- BotoxMedical Patient BrochureDocument21 pagesBotoxMedical Patient BrochurePatricia Avalos C.No ratings yet
- Case Study - Septic ShockDocument16 pagesCase Study - Septic ShockIrene Mae Villanueva Ariola100% (2)
- Aquatic Therapy in RehabilitationDocument28 pagesAquatic Therapy in RehabilitationRadu StoenescuNo ratings yet
- The Nervous System MCQ'sDocument6 pagesThe Nervous System MCQ'sTahir Aziz100% (4)
- Spinal Cord Anatomy MCQ'S: A) Biceps ReflexDocument4 pagesSpinal Cord Anatomy MCQ'S: A) Biceps ReflexTahir Aziz100% (2)
- Introduction To Blood and PhlebotomyDocument149 pagesIntroduction To Blood and PhlebotomyTahir AzizNo ratings yet
- Skeletal System MCQsDocument4 pagesSkeletal System MCQsTahir Aziz100% (3)
- School Nursing ServicesDocument22 pagesSchool Nursing ServicesJimmellee EllenNo ratings yet
- Anatomy: Axial Skeleton MCQS: C SphenoidDocument8 pagesAnatomy: Axial Skeleton MCQS: C SphenoidTahir Aziz50% (2)
- Nursing Care of The Postpartum ClientDocument13 pagesNursing Care of The Postpartum ClientLyca Mae AurelioNo ratings yet
- Climate Change and Resilient Food Systems: Vinaya Kumar Hebsale Mallappa Mahantesh Shirur EditorsDocument423 pagesClimate Change and Resilient Food Systems: Vinaya Kumar Hebsale Mallappa Mahantesh Shirur EditorsDHANARAJA D FOOD TECH (RESEARCH SCHOLAR)No ratings yet
- Hemodynamic Disorders Thrombosis and Shock MCQS2Document4 pagesHemodynamic Disorders Thrombosis and Shock MCQS2Tahir AzizNo ratings yet
- Journals and Reflective Writing: Aims of The ChapterDocument22 pagesJournals and Reflective Writing: Aims of The ChapterTahir AzizNo ratings yet
- Postpartum Sexual Functioning and Its Predicting Factors Among Iranian WomenDocument10 pagesPostpartum Sexual Functioning and Its Predicting Factors Among Iranian WomenTahir AzizNo ratings yet
- My Personal Journal: For Adult Substance UseDocument4 pagesMy Personal Journal: For Adult Substance UseTahir AzizNo ratings yet
- Cerebellum MCQ'S: A) Posterior LobeDocument2 pagesCerebellum MCQ'S: A) Posterior LobeTahir AzizNo ratings yet
- George H. Bishop, Ph. D.: The Present Discussion Deals With Skin Sensation, But Several Facts NeedDocument12 pagesGeorge H. Bishop, Ph. D.: The Present Discussion Deals With Skin Sensation, But Several Facts NeedTahir AzizNo ratings yet
- Skeletal System Introduction and The Axial SkeletonDocument3 pagesSkeletal System Introduction and The Axial SkeletonTahir AzizNo ratings yet
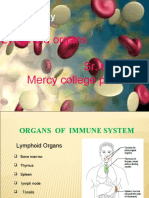
- Immunology: Lymphoid Organs Sr. Sarupya Mercy College PalakkadDocument28 pagesImmunology: Lymphoid Organs Sr. Sarupya Mercy College PalakkadTahir AzizNo ratings yet
- Autonomic Nervous SystemDocument68 pagesAutonomic Nervous SystemTahir AzizNo ratings yet
- Materi SambilotoDocument11 pagesMateri SambilotoArdana MegaNo ratings yet
- Native American Smoking - Campaign Ad #1Document3 pagesNative American Smoking - Campaign Ad #1Haley ReviereNo ratings yet
- Motivation Day 1Document53 pagesMotivation Day 1sambaNo ratings yet
- HFOV - Dragonfly - The Next Primary Mode of Neonatal VentilationDocument16 pagesHFOV - Dragonfly - The Next Primary Mode of Neonatal VentilationflowlineNo ratings yet
- Low Vision: Care of The Patient WithDocument39 pagesLow Vision: Care of The Patient WithDattatri ReddyNo ratings yet
- Dancing With The HungerDocument85 pagesDancing With The HungerJohn McLean100% (1)
- Chapter One 1.0 Introduction/Literature Review 1.1 Background of StudyDocument62 pagesChapter One 1.0 Introduction/Literature Review 1.1 Background of StudySolomonNo ratings yet
- Statistics Related To Child Health.Document34 pagesStatistics Related To Child Health.charan pooniaNo ratings yet
- Lung Volumes and CapacitiesDocument13 pagesLung Volumes and CapacitiesTanmayee MuppaneniNo ratings yet
- Cancer: An Overview: Academic Journal of Cancer Research January 2015Document10 pagesCancer: An Overview: Academic Journal of Cancer Research January 2015Thesis Writing Services and Research InstituteNo ratings yet
- What Are The Possible Causes of DyspneaDocument9 pagesWhat Are The Possible Causes of DyspneaHanis Afiqah Violet MeowNo ratings yet
- Peritoneal Cavity Anatomy in CT PeritoneographyDocument24 pagesPeritoneal Cavity Anatomy in CT PeritoneographyHugo Alberto C FNo ratings yet
- Likelihood Prediction of Diabetes at Early Stage Using Data Mining TechniquesDocument13 pagesLikelihood Prediction of Diabetes at Early Stage Using Data Mining TechniquesOm PandeyNo ratings yet
- Asa Physical Status Classification SystemDocument2 pagesAsa Physical Status Classification SystemDerilandry Isham Aprildhy100% (1)
- Best Practices in Renal Dosing: Bruce A. Mueller, PharmdDocument47 pagesBest Practices in Renal Dosing: Bruce A. Mueller, PharmdRuqayya AdamuNo ratings yet
- Classification: HypertensionDocument13 pagesClassification: HypertensiontermskipopNo ratings yet
- ECPE Cloze Practice TestDocument5 pagesECPE Cloze Practice TestJenny KartNo ratings yet
- Eggplant: January 2013Document29 pagesEggplant: January 2013Gheța AlexandruNo ratings yet
- UTSOE-Journal Vol 5 T 9 PDFDocument74 pagesUTSOE-Journal Vol 5 T 9 PDFAdela AlarcónNo ratings yet
- Guidelines For The Inclusion of Rapid Antigen TestDocument55 pagesGuidelines For The Inclusion of Rapid Antigen TestJm CayabyabNo ratings yet
- IV Complications Ward ClassDocument28 pagesIV Complications Ward ClassMel Belisario TubeoNo ratings yet