You might also like
- Disorders of The BoneDocument31 pagesDisorders of The BoneAyeshaNo ratings yet
- Disorders of The Bone1Document51 pagesDisorders of The Bone1AyeshaNo ratings yet
- Disorders of The BoneDocument35 pagesDisorders of The BoneAyeshaNo ratings yet
- Disorders of The Bone2Document46 pagesDisorders of The Bone2AyeshaNo ratings yet
- Fibrous Dysplasia 29.8.2023Document99 pagesFibrous Dysplasia 29.8.2023Maha JabeenNo ratings yet
- Fibro Osseous LesionsDocument42 pagesFibro Osseous LesionsRose DawoudNo ratings yet
- Radiopacitiesofjaws 160229165805 160916155535 1Document63 pagesRadiopacitiesofjaws 160229165805 160916155535 1mohamedNo ratings yet
- Presentation ON Fibrous Dysplasia: Made by Dr. Waqas Iqbal MDS in Oral PathologyDocument47 pagesPresentation ON Fibrous Dysplasia: Made by Dr. Waqas Iqbal MDS in Oral PathologyWaqas IqbalNo ratings yet
- Diseases of Bone & OsteodystrophiesDocument54 pagesDiseases of Bone & OsteodystrophiesShreya singhNo ratings yet
- L64 Tumor-Like Lesions of BoneDocument19 pagesL64 Tumor-Like Lesions of Bone8ht2twrg5fNo ratings yet
- Maxillofacial Fibro-Osseous LesionsDocument30 pagesMaxillofacial Fibro-Osseous Lesionsnaidu.harikaa15No ratings yet
- Diseasesofboneandhistology 141211233452 Conversion Gate01Document218 pagesDiseasesofboneandhistology 141211233452 Conversion Gate01JuhiJahan AmanullahNo ratings yet
- CystsDocument27 pagesCystspasser byNo ratings yet
- Bone DiseasesDocument191 pagesBone DiseasesDrRobin SabharwalNo ratings yet
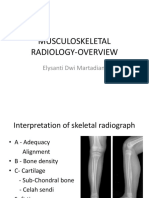
- Musculoskeletal Radiology-Overview: Elysanti Dwi MartadianiDocument42 pagesMusculoskeletal Radiology-Overview: Elysanti Dwi MartadianiRisma Ari PertiwiNo ratings yet
- Fibro OsseousDocument25 pagesFibro OsseoussadiaNo ratings yet
- Fibous DysplasiaDocument24 pagesFibous DysplasiaLisa MoyoNo ratings yet
- Ossifying FibromaDocument22 pagesOssifying FibromaMaha JabeenNo ratings yet
- Osteochondroma: Dr. Mahesh Chaudhary Phase-A Resident Radiology & Imaging BsmmuDocument36 pagesOsteochondroma: Dr. Mahesh Chaudhary Phase-A Resident Radiology & Imaging BsmmubucculuNo ratings yet
- Benign Odontogenic Tumou1rDocument67 pagesBenign Odontogenic Tumou1rVISHAL DHIMANNo ratings yet
- Disease of Bone Manifested in The JawsDocument35 pagesDisease of Bone Manifested in The Jawsyongky100% (1)
- Fibrous DysplasiaDocument2 pagesFibrous DysplasiaGus SwanjayaNo ratings yet
- Mixed Lesions ImagingDocument33 pagesMixed Lesions ImagingAdamNo ratings yet
- ContentDocument48 pagesContentRajat Nangia100% (1)
- Fibro Osseous LesionsDocument50 pagesFibro Osseous LesionsanviNo ratings yet
- Benign Nonodontogenic TumorsDocument20 pagesBenign Nonodontogenic TumorsEuginia YosephineNo ratings yet
- Bone Tumours - I & Ii - 2015Document113 pagesBone Tumours - I & Ii - 2015Nur Atiqah Mohd AzliNo ratings yet
- Differential Diagnosis of Periapical RadiopacitiesDocument19 pagesDifferential Diagnosis of Periapical RadiopacitiesNaishadh DalalNo ratings yet
- Seminar W4 - Bone & Soft Tissue TumoursDocument123 pagesSeminar W4 - Bone & Soft Tissue TumoursUN EPNo ratings yet
- OsteopetrosisDocument13 pagesOsteopetrosisDeep SavaliaNo ratings yet
- Important Tables of Oral PathologyDocument17 pagesImportant Tables of Oral PathologyEasy Med LecturesNo ratings yet
- BONE LOSS AND PATTERNS OF BONE DESTRUCTION HDocument33 pagesBONE LOSS AND PATTERNS OF BONE DESTRUCTION Heimaan afrozNo ratings yet
- Fibro-Osseus LesionsDocument56 pagesFibro-Osseus LesionsyomanNo ratings yet
- One Tumours Fibrous Tumours: Prof. R. N .Srivastav Dr. Anil PandaDocument40 pagesOne Tumours Fibrous Tumours: Prof. R. N .Srivastav Dr. Anil PandaNaysahNo ratings yet
- Fibroosseous LesionsDocument28 pagesFibroosseous LesionsDr'Paramjot KaurNo ratings yet
- Cystic Bone LesionsDocument47 pagesCystic Bone LesionsAnwar KhanNo ratings yet
- Bone TumorsDocument27 pagesBone Tumorsaliaz duxNo ratings yet
- Osteochondroma 150907182521 Lva1 App6891Document22 pagesOsteochondroma 150907182521 Lva1 App6891bucculuNo ratings yet
- BONE - 09 - Bone TumorsDocument68 pagesBONE - 09 - Bone TumorsAmrit GautamNo ratings yet
- OsteomyelitisDocument91 pagesOsteomyelitisamenNo ratings yet
- Resective Osseous SurgeryDocument57 pagesResective Osseous SurgeryМихаил Танев100% (1)
- Edition CH #23 Other Bone Diseases: Stuart C. White & Michael J. PharoahDocument21 pagesEdition CH #23 Other Bone Diseases: Stuart C. White & Michael J. PharoahPrince AhmedNo ratings yet
- Bone Destruction and TypeDocument51 pagesBone Destruction and TypeHuyền LêNo ratings yet
- 12) Cystic Lesions of BoneDocument18 pages12) Cystic Lesions of BonesarathNo ratings yet
- Guía Radio Buco IIIDocument26 pagesGuía Radio Buco IIIRicardo GonzalezNo ratings yet
- UntitledDocument56 pagesUntitledDinesh YadavNo ratings yet
- Fibro-Osseous Lesions and Benign Tumors of The JawDocument103 pagesFibro-Osseous Lesions and Benign Tumors of The JawJomi PorinchuNo ratings yet
- Wa0027.Document31 pagesWa0027.apdallahyousef11No ratings yet
- Lumps and Swellings in The Jaws: Aneurysmal Bone CystDocument4 pagesLumps and Swellings in The Jaws: Aneurysmal Bone CystGokul SivaNo ratings yet
- ONCOLOGYDocument23 pagesONCOLOGYJoanna Mae ShawyerNo ratings yet
- Oral Path I CombinedDocument68 pagesOral Path I CombinedkmcalleNo ratings yet
- Zebra XX, Part 2 PDFDocument3 pagesZebra XX, Part 2 PDFRamona MateiNo ratings yet
- ABCDEF Approach To Radiographic Analysis of Bone TumorsDocument37 pagesABCDEF Approach To Radiographic Analysis of Bone Tumorsprashanth nagarajNo ratings yet
- Wa0027.Document29 pagesWa0027.apdallahyousef11No ratings yet
- Giant Cell Rich Lesions of BoneDocument151 pagesGiant Cell Rich Lesions of BoneNikhita JosyNo ratings yet
- Interpretasi Lesi SpesifikDocument27 pagesInterpretasi Lesi SpesifikSTEFFI MIFTANo ratings yet
- Topics: Fibrous Dysplasia, Cemento-Osseus Dysplasia Submitted By: Pooja ChaturvediDocument48 pagesTopics: Fibrous Dysplasia, Cemento-Osseus Dysplasia Submitted By: Pooja ChaturvediRajat DabholkarNo ratings yet
- Osteomyelitis RadiologyDocument26 pagesOsteomyelitis RadiologySheila Mae CabahugNo ratings yet
- The Globalization of Cemex: Case Analysis - International BusinessDocument5 pagesThe Globalization of Cemex: Case Analysis - International BusinessHimanshu KumarNo ratings yet
- Cemex GlobalisationDocument5 pagesCemex GlobalisationHighland Vn100% (3)
- Analysis of Cemex'S Strategies As Determinants For Market PowerDocument8 pagesAnalysis of Cemex'S Strategies As Determinants For Market PowerAyeshaNo ratings yet
- CEMEXDocument4 pagesCEMEXRyanNo ratings yet
- Case Study Analysis GbeDocument4 pagesCase Study Analysis GbeSaif Ul IslamNo ratings yet
- Cemex CaseDocument3 pagesCemex CaseRohit Jain100% (1)
- Sterilization and Cross Infection ControlDocument27 pagesSterilization and Cross Infection ControlAyeshaNo ratings yet
- Zygomatic ComplexDocument21 pagesZygomatic ComplexAyeshaNo ratings yet
- Diagnosis and Management of Odontogenic InfectionsDocument52 pagesDiagnosis and Management of Odontogenic InfectionsAhmed EmadNo ratings yet
- Odontogenic InfectionDocument73 pagesOdontogenic InfectionAyeshaNo ratings yet
- 8.aseptic TechniquesDocument24 pages8.aseptic TechniquesAyeshaNo ratings yet
- Oral Care of Patients Undergoing Chemotherapy andDocument24 pagesOral Care of Patients Undergoing Chemotherapy andAyeshaNo ratings yet
- Chronic Infections of Jaws OR Inflammator Diseases of BoneDocument43 pagesChronic Infections of Jaws OR Inflammator Diseases of BoneAyeshaNo ratings yet
- Mandibular FracturesDocument42 pagesMandibular FracturesAyeshaNo ratings yet
- Maxillary FracturesDocument18 pagesMaxillary FracturesAyeshaNo ratings yet
- Local Anesthesia Techniques For ChildrenDocument33 pagesLocal Anesthesia Techniques For ChildrenAyeshaNo ratings yet
- Exo ComplicationsDocument18 pagesExo ComplicationsAyeshaNo ratings yet
- Facial FracturesDocument35 pagesFacial FracturesmanianniNo ratings yet
- Intervelar-Veloplasty (Pharyngoplasty)Document18 pagesIntervelar-Veloplasty (Pharyngoplasty)AyeshaNo ratings yet
- Lefort 1 OstoetomyDocument35 pagesLefort 1 OstoetomyAyeshaNo ratings yet
- Endocrine and Metabolic DisordersDocument21 pagesEndocrine and Metabolic DisordersAyeshaNo ratings yet
- Endocrine and Metabolic DisordersDocument21 pagesEndocrine and Metabolic DisordersAyeshaNo ratings yet
- Disorders of The Bone FynalDocument69 pagesDisorders of The Bone FynalAyeshaNo ratings yet
- Embryo 11ADocument85 pagesEmbryo 11AAyeshaNo ratings yet
- Disorders of The Bone FynalDocument69 pagesDisorders of The Bone FynalAyeshaNo ratings yet
- English For Nurse 5: 5. Reading Unit A. MR Jansen Has Had A Myocardial InfarctionDocument4 pagesEnglish For Nurse 5: 5. Reading Unit A. MR Jansen Has Had A Myocardial InfarctiondnnssnNo ratings yet
- Physical Activity and Active RecreationDocument38 pagesPhysical Activity and Active Recreationivan hernandezNo ratings yet
- The Management of Seborrheic Dermatitis 2020Document11 pagesThe Management of Seborrheic Dermatitis 2020Sema GigaramadanNo ratings yet
- Medical Certificate (Form 41)Document1 pageMedical Certificate (Form 41)Nasra AbdulganiNo ratings yet
- Hydrocele 1Document2 pagesHydrocele 1Mella IntaniabellaNo ratings yet
- QiGong Global SummitDocument45 pagesQiGong Global SummittoanomisNo ratings yet
- Assignment On: Bio-PreservationDocument18 pagesAssignment On: Bio-PreservationtowhidNo ratings yet
- Prevenção Secundária Avc Isquêmico - Guideline 2022Document41 pagesPrevenção Secundária Avc Isquêmico - Guideline 2022Felipe Stoquetti de AbreuNo ratings yet
- Rash and Fever After Sulfasalazine UseDocument5 pagesRash and Fever After Sulfasalazine UseChistian LassoNo ratings yet
- Children Hypertension ChartDocument4 pagesChildren Hypertension ChartHo Yoke MeiNo ratings yet
- Commonly Billed Codes: Spinal Cord StimulationDocument21 pagesCommonly Billed Codes: Spinal Cord StimulationKrishna KumarNo ratings yet
- Drugs Acting On The Autonomic Nervous SystemDocument68 pagesDrugs Acting On The Autonomic Nervous SystemjisooNo ratings yet
- Epidemiology: Chapter 1: IntroductionDocument134 pagesEpidemiology: Chapter 1: IntroductionLoai Mohammed IssaNo ratings yet
- GK For Veterinary PDFDocument20 pagesGK For Veterinary PDFMohammed AdilNo ratings yet
- Medical Parasitology A Self Instructional Text PDFDriveDocument60 pagesMedical Parasitology A Self Instructional Text PDFDriveDenise Sta. AnaNo ratings yet
- Managing Teen Stress: December 2015Document11 pagesManaging Teen Stress: December 2015Lan TrầnNo ratings yet
- Problem StatementDocument18 pagesProblem StatementvmrekhateNo ratings yet
- Procalcitonin GuidanceDocument44 pagesProcalcitonin GuidanceMiguel Chung SangNo ratings yet
- Genitourinary TuberculosisDocument10 pagesGenitourinary TuberculosisMrunal DiveNo ratings yet
- Disorders of The EarDocument8 pagesDisorders of The EarVinz Khyl G. CastillonNo ratings yet
- 6.2 Diabetes MellitusDocument53 pages6.2 Diabetes MellitusMohammad AlrefaiNo ratings yet
- Week 6 - Antiparkinsonism AgentsDocument18 pagesWeek 6 - Antiparkinsonism AgentsDino MicaNo ratings yet
- Congenital Anomalies of KidneDocument7 pagesCongenital Anomalies of KidneSanthosh.S.U100% (2)
- Principales Fluidos y Secreciones de Análisis en LaboratorioDocument34 pagesPrincipales Fluidos y Secreciones de Análisis en LaboratorioDennis Lorena Cárdenas LealNo ratings yet
- Case Files® EnterococcusDocument4 pagesCase Files® EnterococcusAHMAD ADE SAPUTRANo ratings yet
- Clinical Congress: ProgramDocument15 pagesClinical Congress: ProgramErlan SantosNo ratings yet
- (Neurology) 2 - Vascular SystemDocument6 pages(Neurology) 2 - Vascular SystemChristine LopezNo ratings yet
- Chapter 20 Admission, Transfer, and DischargeDocument4 pagesChapter 20 Admission, Transfer, and DischargetvrossyNo ratings yet
- Eisenmenger Syndrome: Clinical DefinitionDocument3 pagesEisenmenger Syndrome: Clinical Definition22194No ratings yet
- Heart Dysrhythmias Cheat Sheet PDFDocument5 pagesHeart Dysrhythmias Cheat Sheet PDFbarbaraNo ratings yet