You might also like
- Acls Manual PDFDocument30 pagesAcls Manual PDFCyner Cruz100% (2)
- Avant Review Lesson 1-8 ECG Rhythm Strip InterpretationDocument28 pagesAvant Review Lesson 1-8 ECG Rhythm Strip InterpretationphoebjaetanNo ratings yet
- Electro Cardiogram & DysrythmiasDocument40 pagesElectro Cardiogram & DysrythmiasshobharamkrishnaNo ratings yet
- SyncopeDocument105 pagesSyncopeJohn DasNo ratings yet
- Dysrhythmia Recognition Pocket Reference Card PDFDocument14 pagesDysrhythmia Recognition Pocket Reference Card PDFjenn1722100% (2)
- ACLS Pre-TestDocument24 pagesACLS Pre-TestBaltej Sidhu80% (10)
- ECG Rhythm Strip Interpretation Lesson 4Document5 pagesECG Rhythm Strip Interpretation Lesson 4phoebjaetanNo ratings yet
- Cardiology Study Guide Handout PDFDocument86 pagesCardiology Study Guide Handout PDFStarr Newman100% (1)
- Cardiovascular Physiology 2Document52 pagesCardiovascular Physiology 2maxmus4No ratings yet
- Lecture 4 - Circulatory SystemDocument83 pagesLecture 4 - Circulatory Systemnuleka thulminiNo ratings yet
- ArrhthmiasDocument44 pagesArrhthmiasmadeha goharNo ratings yet
- Cardiac Conduction: Shoiab AlamDocument26 pagesCardiac Conduction: Shoiab AlamUzma KhanNo ratings yet
- Cardiovascular Physiology 1Document44 pagesCardiovascular Physiology 1maxmus4No ratings yet
- Arrhythmia Clinical PracticeDocument12 pagesArrhythmia Clinical PracticeSaba ElmahadiNo ratings yet
- Electrocardiogram: By: Keverne Jhay P. Colas, RN, MANDocument72 pagesElectrocardiogram: By: Keverne Jhay P. Colas, RN, MANGaras AnnaBerniceNo ratings yet
- Nursing School EKGDocument43 pagesNursing School EKGRob Dickerson100% (1)
- Arrythemia 1Document73 pagesArrythemia 1Mooma fatimaNo ratings yet
- Arrhythmias: Anurag Patidar Lecturer, Con, DMCHDocument40 pagesArrhythmias: Anurag Patidar Lecturer, Con, DMCHpreet kaurNo ratings yet
- Prof DR Najneen AkhterDocument62 pagesProf DR Najneen Akhterislamamirul0487No ratings yet
- Cardiac ArrythmiasDocument24 pagesCardiac ArrythmiasAejaz AhmadNo ratings yet
- EkgDocument94 pagesEkgCaprita LauraNo ratings yet
- Cardiac Cycle and Myogenic Control of HeartbeatDocument25 pagesCardiac Cycle and Myogenic Control of HeartbeatFiona HennahNo ratings yet
- Dr. Niranjan Murthy HL Associate Professor Dept of Physiology SSMC, TumkurDocument53 pagesDr. Niranjan Murthy HL Associate Professor Dept of Physiology SSMC, TumkurnirilibNo ratings yet
- Conducting System of The HeartDocument27 pagesConducting System of The HeartMuhammadNo ratings yet
- 1.1 CV PhysiologyDocument34 pages1.1 CV PhysiologygilangbpNo ratings yet
- ECG3Document58 pagesECG3Plzstudylav SyedNo ratings yet
- Electrocardiogram: Hanan Fathy 2008Document94 pagesElectrocardiogram: Hanan Fathy 2008LiliLiliNo ratings yet
- Advanced ECG AnalysisDocument90 pagesAdvanced ECG AnalysisnursewinstonNo ratings yet
- Cardiac PacemakersDocument49 pagesCardiac PacemakersMohammad AliNo ratings yet
- Cadiac Cycle, Heart Sound, ECG, HypertensionDocument110 pagesCadiac Cycle, Heart Sound, ECG, HypertensionNilesh100% (1)
- 05 Cardiovascular System PhysiologyDocument34 pages05 Cardiovascular System PhysiologyKaye Alyssa EnriquezNo ratings yet
- Conducting System of HeartDocument13 pagesConducting System of HeartAdam PrabowoNo ratings yet
- Origin & Conduction of Cardiac Impulse: Dr.S.Brinda MD Associate Professor PhysiologyDocument36 pagesOrigin & Conduction of Cardiac Impulse: Dr.S.Brinda MD Associate Professor PhysiologyAtchaya ThillainatarajanNo ratings yet
- Cardiac Arrhythmia From Guyton's BookDocument10 pagesCardiac Arrhythmia From Guyton's BookNadhirah Mohamad NohNo ratings yet
- ECGDocument44 pagesECGJay ItaliyaNo ratings yet
- CardiovascularDocument40 pagesCardiovascularÁñèsh Kåøs100% (1)
- ECG ECG Basics Presentation 201309101527422446 PDFDocument45 pagesECG ECG Basics Presentation 201309101527422446 PDFRamesh RajNo ratings yet
- Arrhythmias 101Document59 pagesArrhythmias 101Abdiwahab ShahnizzleNo ratings yet
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocument50 pagesCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNo ratings yet
- Cardiology Ebook Notes PDFDocument26 pagesCardiology Ebook Notes PDFsugisweNo ratings yet
- 321 Lecture ECGDocument38 pages321 Lecture ECGCea Mikee Mitch BartolomeNo ratings yet
- 3rd Lecture On Arrythmias by Dr. RoomiDocument16 pages3rd Lecture On Arrythmias by Dr. RoomiMudassar Roomi100% (2)
- ArrhythmiaDocument29 pagesArrhythmiaMohamed Hassan MohamudNo ratings yet
- 11 Ant HEART MUSCLEDocument57 pages11 Ant HEART MUSCLEZuhaib AhmedNo ratings yet
- Cardiac Arrhythmia 171209212142 2Document74 pagesCardiac Arrhythmia 171209212142 2Gunel Sadiqova100% (1)
- Electrocardiography (Ecg) : Presented By: Fahad I. HussienDocument102 pagesElectrocardiography (Ecg) : Presented By: Fahad I. HussienMustafa A. DawoodNo ratings yet
- 22 Disritmia 2018Document60 pages22 Disritmia 2018Nur akilaNo ratings yet
- Anatomi Fisiologi Sistem Kardiovaskuler 1Document52 pagesAnatomi Fisiologi Sistem Kardiovaskuler 1Vaweli Putri Spelman DpNo ratings yet
- Tomasz WikarekDocument95 pagesTomasz Wikareknamar13766No ratings yet
- EEG ContdDocument50 pagesEEG ContdBulkiesNo ratings yet
- Cardiac Muscle and Heart FunctionDocument22 pagesCardiac Muscle and Heart FunctionFransiska Anggreni SihotangNo ratings yet
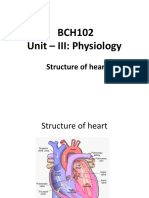
- BCH102 Unit - III: Physiology: Structure of HeartDocument17 pagesBCH102 Unit - III: Physiology: Structure of Heartdivya vajpayeeNo ratings yet
- Dysrhythmia PowerpointDocument10 pagesDysrhythmia PowerpointWynton De JesusNo ratings yet
- Lecture5 - Electrocardiogram Electromyogram - 1Document33 pagesLecture5 - Electrocardiogram Electromyogram - 1AbdullahNo ratings yet
- Cardia Arrhythmias Zuket 3.0Document68 pagesCardia Arrhythmias Zuket 3.0Mohd ZulkhairiNo ratings yet
- Physiology of HeartDocument74 pagesPhysiology of Heartmadeha goharNo ratings yet
- 4 - PHYSIOLOGY - Electrical Activity of The Heart LectureDocument78 pages4 - PHYSIOLOGY - Electrical Activity of The Heart Lecturefznfbw8qqcNo ratings yet
- Core V - Cardiovascular CoreDocument35 pagesCore V - Cardiovascular CoreMatthew LeiNo ratings yet
- Ecg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HDocument69 pagesEcg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HRohini RaiNo ratings yet
- Mechanisme ArrhythmiaDocument38 pagesMechanisme ArrhythmiarskdemergencyNo ratings yet
- An Introduction To The 12 Lead EcgDocument85 pagesAn Introduction To The 12 Lead EcgAris Diyan YulistiawanNo ratings yet
- Electrocardioghraphy ECG/ (EKG) : ZTG PHR 327 Fall 2019Document17 pagesElectrocardioghraphy ECG/ (EKG) : ZTG PHR 327 Fall 2019mujNo ratings yet
- Cardiovascular AlterationsDocument46 pagesCardiovascular Alterationsaneesnair86No ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Transport of Carbon DioxideDocument17 pagesTransport of Carbon Dioxideyasir ishaqNo ratings yet
- Transport of Carbon DioxideDocument17 pagesTransport of Carbon Dioxideyasir ishaqNo ratings yet
- Body Heat During ExerciseDocument24 pagesBody Heat During Exerciseyasir ishaq100% (1)
- Circulation J Pressure J Flow and Resistance of by YasirDocument47 pagesCirculation J Pressure J Flow and Resistance of by Yasiryasir ishaqNo ratings yet
- Beta Cell de Differtiation & Trans DiffertiationDocument6 pagesBeta Cell de Differtiation & Trans Differtiationyasir ishaqNo ratings yet
- The Clinical Anatomy of The Crista Terminalis, Pectinate Muscles and The Teniae SagittalisDocument7 pagesThe Clinical Anatomy of The Crista Terminalis, Pectinate Muscles and The Teniae SagittalisSandro PinhoNo ratings yet
- Fuster Et Al 2001 Acc Aha Esc Guidelines For The Management of Patients With Atrial Fibrillation Executive Summary ADocument33 pagesFuster Et Al 2001 Acc Aha Esc Guidelines For The Management of Patients With Atrial Fibrillation Executive Summary AAlfita RahmawatiNo ratings yet
- The Six Second ECG: Annotated Answer KeyDocument9 pagesThe Six Second ECG: Annotated Answer KeyShimika Tomes100% (1)
- Jurnal Aritmia 1Document6 pagesJurnal Aritmia 1Aprilia Fani PNo ratings yet
- Acls Algorithms 2012Document12 pagesAcls Algorithms 2012kivuNo ratings yet
- Pre-Excitation Syndromes in Children: Dr.K.MaheshDocument105 pagesPre-Excitation Syndromes in Children: Dr.K.MaheshNischal ShahNo ratings yet
- Normal Sinus RhythmDocument8 pagesNormal Sinus RhythmRosalyn YuNo ratings yet
- 2020 AFIB 2020 - For WebDocument166 pages2020 AFIB 2020 - For WebHussein TfNo ratings yet
- SVTDocument8 pagesSVTJulieNo ratings yet
- Chapter 1 ECGDocument67 pagesChapter 1 ECGAnton BalansagNo ratings yet
- Tutorial On Electrophysiology of The Heart) Sam Dudley, Brown UniversityDocument50 pagesTutorial On Electrophysiology of The Heart) Sam Dudley, Brown UniversityNavojit ChowdhuryNo ratings yet
- European Journal of Internal MedicineDocument4 pagesEuropean Journal of Internal Medicinesamer battatNo ratings yet
- Algoritma SVTDocument87 pagesAlgoritma SVTbonne_ameNo ratings yet
- Arritmias en El EmbarazoDocument10 pagesArritmias en El EmbarazoJuan Soto FarfanNo ratings yet
- STRONG-HF TrialDocument16 pagesSTRONG-HF TrialyukeNo ratings yet
- ARITMIA, Gangguan Irama JantungDocument37 pagesARITMIA, Gangguan Irama JantungNovriefta NugrahaNo ratings yet
- NCM 118 RLE (Week 7-8)Document7 pagesNCM 118 RLE (Week 7-8)kNo ratings yet
- Disorders of Cardiac RhythmDocument66 pagesDisorders of Cardiac RhythmslyfoxkittyNo ratings yet
- PPP v3Document771 pagesPPP v3Steven Lam100% (1)
- Tematica Licenta 2012 2013 FMF Oradea Medicina in Limba EnglezaDocument3 pagesTematica Licenta 2012 2013 FMF Oradea Medicina in Limba EnglezaLacramioara_Te_3375No ratings yet
- k.41 ATRIAL FLUTTERDocument8 pagesk.41 ATRIAL FLUTTERjamaliganteng88No ratings yet
- PVC Unido ConDuplicadosDocument1,181 pagesPVC Unido ConDuplicadosJorge Chachaima MarNo ratings yet
- Resident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)Document104 pagesResident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)scalixto100% (1)
- ECG Physician's Guide (Japanese)Document49 pagesECG Physician's Guide (Japanese)Mohammad NasriNo ratings yet