You might also like
- Psychiatric History and Mental Status ExaminationDocument24 pagesPsychiatric History and Mental Status ExaminationLinus PuleNo ratings yet
- Psychiatry Chapter 3Document54 pagesPsychiatry Chapter 3Online Money In EthiopiaNo ratings yet
- History and Exam With DescriptionDocument10 pagesHistory and Exam With Descriptionmedicine lifeNo ratings yet
- Psychiatric Interview Kap ExtDocument61 pagesPsychiatric Interview Kap ExtNeba YenatuNo ratings yet
- The Effect of Meditation and Relaxation on Individuals Diagnosed with Long-Term SchizophreniaFrom EverandThe Effect of Meditation and Relaxation on Individuals Diagnosed with Long-Term SchizophreniaNo ratings yet
- Detailed Assessment in Clinical PracticeDocument22 pagesDetailed Assessment in Clinical PracticeAdamu GudinaNo ratings yet
- Case Presentation StyleDocument7 pagesCase Presentation StyleNiteshSinghNo ratings yet
- By Ethel Maureen B. Pagaddu, MDDocument49 pagesBy Ethel Maureen B. Pagaddu, MDRyan James Lorenzo MiguelNo ratings yet
- Mental Status Examination - Bring To LectureDocument6 pagesMental Status Examination - Bring To LectureJae ChoiNo ratings yet
- Anxiety: Adolescent Patients - CE: AlertDocument10 pagesAnxiety: Adolescent Patients - CE: AlertircomfarNo ratings yet
- Chapter 15 - Health and Physical Assessment of The Adult ClientDocument65 pagesChapter 15 - Health and Physical Assessment of The Adult ClientKristian Jane de Jesus100% (1)
- The Silent Cry Understanding Children's Struggle With Self-Harm, Overcoming Pain And Building ResilienceFrom EverandThe Silent Cry Understanding Children's Struggle With Self-Harm, Overcoming Pain And Building ResilienceNo ratings yet
- Assessment of an Ill PatientDocument69 pagesAssessment of an Ill PatientEvancemwenya123No ratings yet
- Mayer Gross History Taking and MSE ProformaDocument13 pagesMayer Gross History Taking and MSE ProformaHimanshi ShokeenNo ratings yet
- Interview: Patient HistoryDocument8 pagesInterview: Patient HistoryquelspectacleNo ratings yet
- Living Recovery: Youth Speak Out on “Owning” Mental IllnessFrom EverandLiving Recovery: Youth Speak Out on “Owning” Mental IllnessNo ratings yet
- The Emotional Causes of Diseases: A Mind Body PerspectiveFrom EverandThe Emotional Causes of Diseases: A Mind Body PerspectiveNo ratings yet
- The Psychiatric History and Mental State ExaminationDocument2 pagesThe Psychiatric History and Mental State ExaminationEma100% (1)
- Coping with Bipolar Disorder: A CBT-Informed Guide to Living with Manic DepressionFrom EverandCoping with Bipolar Disorder: A CBT-Informed Guide to Living with Manic DepressionNo ratings yet
- Tom's Fourth Year Guide (2011-12)Document709 pagesTom's Fourth Year Guide (2011-12)jangyNo ratings yet
- Behavioral Health PrepDocument32 pagesBehavioral Health PrepStarr NewmanNo ratings yet
- Psychological Report Writing: Adapted From UP-PGH FormatDocument22 pagesPsychological Report Writing: Adapted From UP-PGH FormatAhmad AliNo ratings yet
- Psychiatric Interview Module 1Document41 pagesPsychiatric Interview Module 1Spj Bernardo100% (1)
- Gale Researcher Guide for: Overview of Behavioral and Mental Disorders in PsychologyFrom EverandGale Researcher Guide for: Overview of Behavioral and Mental Disorders in PsychologyNo ratings yet
- Interview in PsychiatryDocument34 pagesInterview in PsychiatryEthiopia TekdemNo ratings yet
- Psychiatric Assessment OutlineDocument3 pagesPsychiatric Assessment OutlineRuksNo ratings yet
- Appearance and General BehaviorDocument3 pagesAppearance and General BehaviorHardeep KaurNo ratings yet
- MENTAL HEALTH NURSING ExamDocument5 pagesMENTAL HEALTH NURSING ExamSurkhali BipanaNo ratings yet
- Pathways to Recovery: Preventing Relapse in First Episode Psychosis: Strategies for Relapse Prevention and Mental Health Resilience in First Episode PsychosisFrom EverandPathways to Recovery: Preventing Relapse in First Episode Psychosis: Strategies for Relapse Prevention and Mental Health Resilience in First Episode PsychosisNo ratings yet
- Mental Health Recovery: Can Prayer Cure Mental Illness? Can people fully recover from mental illness ?From EverandMental Health Recovery: Can Prayer Cure Mental Illness? Can people fully recover from mental illness ?Rating: 5 out of 5 stars5/5 (1)
- OPIANA CHRISTIAN JOSEPH - ReseachAssignmentDocument16 pagesOPIANA CHRISTIAN JOSEPH - ReseachAssignmentChristian Joseph OpianaNo ratings yet
- Weathering the Storm: A Guide to Understanding and Overcoming Mood DisordersFrom EverandWeathering the Storm: A Guide to Understanding and Overcoming Mood DisordersNo ratings yet
- Hearing Voices: Qualitative Inquiry in Early PsychosisFrom EverandHearing Voices: Qualitative Inquiry in Early PsychosisNo ratings yet
- Nourishing Minds: The Interplay of Eating and Mental HealthFrom EverandNourishing Minds: The Interplay of Eating and Mental HealthNo ratings yet
- Holistic Nursing AssessmentDocument8 pagesHolistic Nursing Assessmentandreagonzalooo27No ratings yet
- Introduction To Psychiatric NursingDocument88 pagesIntroduction To Psychiatric NursingMinlik-alew Dejenie100% (1)
- Tulsa Traditional N4043 Exam I Study Guide Fall 2015Document18 pagesTulsa Traditional N4043 Exam I Study Guide Fall 2015Bao NguyenNo ratings yet
- Without Stigma: About the Stigma of the Mental IllnessFrom EverandWithout Stigma: About the Stigma of the Mental IllnessRating: 5 out of 5 stars5/5 (1)
- Psychiatry History Taking FormatDocument7 pagesPsychiatry History Taking Formatavi_ajayNo ratings yet
- Counseling Interview: Strategies & TechniquesDocument52 pagesCounseling Interview: Strategies & TechniquesjerilNo ratings yet
- Coping with Shyness and Social Phobias: A Guide to Understanding and Overcoming Social AnxietyFrom EverandCoping with Shyness and Social Phobias: A Guide to Understanding and Overcoming Social AnxietyRating: 3 out of 5 stars3/5 (1)
- Mental Health-1Document130 pagesMental Health-1Nampamba WinnieNo ratings yet
- Hospice Powerpoint LectureDocument161 pagesHospice Powerpoint LectureFrancis Emman Santiago0% (1)
- How Psychological Health Affects Your Physical Health: Toxic People Are No Good For YouFrom EverandHow Psychological Health Affects Your Physical Health: Toxic People Are No Good For YouNo ratings yet
- Lyceum Northwestern University - FQDMF College of Medicine Dagupan City, PangasinanDocument8 pagesLyceum Northwestern University - FQDMF College of Medicine Dagupan City, PangasinanGowthami GarimellaNo ratings yet
- Narcissistic Fathers an Emotional Abuse Workbook: Narcissistic States and the Therapeutic ProcessFrom EverandNarcissistic Fathers an Emotional Abuse Workbook: Narcissistic States and the Therapeutic ProcessNo ratings yet
- Neeraj AhujaDocument13 pagesNeeraj Ahujaclinicweecare100% (1)
- Behavioural Sciences IntroDocument31 pagesBehavioural Sciences IntroDodo JuniorNo ratings yet
- Psychosocial Assessment Techniques for Psychiatric NursingDocument44 pagesPsychosocial Assessment Techniques for Psychiatric NursingHershey Cordero Briones100% (1)
- Understanding Anxiety: A Guide for Patients, Family, and FriendsFrom EverandUnderstanding Anxiety: A Guide for Patients, Family, and FriendsNo ratings yet
- Case 2 Quiz - Case in OphthalmologyDocument10 pagesCase 2 Quiz - Case in OphthalmologyRakesh KumarNo ratings yet
- Mental Health TalkDocument33 pagesMental Health TalkRakesh KumarNo ratings yet
- Clinical Exam of The Psychiatric PX HX MSE Signs Symptoms Modified For Senior Clerks 2021Document139 pagesClinical Exam of The Psychiatric PX HX MSE Signs Symptoms Modified For Senior Clerks 2021Rakesh KumarNo ratings yet
- OPHTHA: Top Drugs for Eye Exams, Glaucoma, and MoreDocument10 pagesOPHTHA: Top Drugs for Eye Exams, Glaucoma, and MoreRakesh KumarNo ratings yet
- Record The Patient's VATEF: Based On The Data ProvidedDocument19 pagesRecord The Patient's VATEF: Based On The Data ProvidedRakesh KumarNo ratings yet
- Case 2 Quiz - Case in OphthalmologyDocument10 pagesCase 2 Quiz - Case in OphthalmologyRakesh KumarNo ratings yet
- Clinical Exam of The Psychiatric PX HX MSE Signs Symptoms Modified For Senior Clerks 2021Document139 pagesClinical Exam of The Psychiatric PX HX MSE Signs Symptoms Modified For Senior Clerks 2021Rakesh KumarNo ratings yet
- Clinical Exam of The Psychiatric PX HX MSE Signs Symptoms Modified For Senior Clerks 2021Document139 pagesClinical Exam of The Psychiatric PX HX MSE Signs Symptoms Modified For Senior Clerks 2021Rakesh KumarNo ratings yet
- Infectious Gastrointestinal Diseases: MicrobiologyDocument37 pagesInfectious Gastrointestinal Diseases: MicrobiologyRakesh KumarNo ratings yet
- Cold Agglutinin DiseaseDocument32 pagesCold Agglutinin DiseaseRakesh KumarNo ratings yet
- Monument EssayDocument2 pagesMonument EssayLauren RosadoNo ratings yet
- Coping Mechanisms of a Sibling Violence VictimDocument26 pagesCoping Mechanisms of a Sibling Violence VictimYzel SeniningNo ratings yet
- Muktha Foundation - National Conference On IPV - 2023 - CompressedDocument9 pagesMuktha Foundation - National Conference On IPV - 2023 - Compressedshreya sharmaNo ratings yet
- 2020-2021 Course Catalog: Masters and Doctoral Programs in The Tradition of Depth PsychologyDocument249 pages2020-2021 Course Catalog: Masters and Doctoral Programs in The Tradition of Depth PsychologyTelma Regina Ventura100% (1)
- Final Academic PaperDocument3 pagesFinal Academic PaperKristelyn FranciscoNo ratings yet
- Students' Reading Comprehension ImprovementDocument3 pagesStudents' Reading Comprehension ImprovementLisa RLNo ratings yet
- Schindler Chpt1Document24 pagesSchindler Chpt1CharleneKronstedtNo ratings yet
- Practical Qualitative Research: David Cababaro BuenoDocument106 pagesPractical Qualitative Research: David Cababaro BuenoCesar Ian RoaNo ratings yet
- Chapter 5 Memory PsychologyDocument39 pagesChapter 5 Memory PsychologyJupiter BassettNo ratings yet
- EF4e Adv Filetest 05bDocument7 pagesEF4e Adv Filetest 05banaNo ratings yet
- Mscfe 622 Continuous-Time Stochastic Processes - Course SyllabusDocument1 pageMscfe 622 Continuous-Time Stochastic Processes - Course SyllabusAbdullah AbdullahNo ratings yet
- A Female Dog Forced Me To Cum Several TimesDocument7 pagesA Female Dog Forced Me To Cum Several Timeskadas alkadasNo ratings yet
- RRL ProcrastinationDocument7 pagesRRL ProcrastinationAleyah Pionne100% (1)
- XII - Psycho - Sample Paper-2Document12 pagesXII - Psycho - Sample Paper-2shresthachakraborty2005No ratings yet
- Introduction of A Research PaperDocument5 pagesIntroduction of A Research Paperegabnlrhf100% (1)
- Thaddius Barker - The Book of Whichcraft PDFDocument45 pagesThaddius Barker - The Book of Whichcraft PDFFreddie666100% (2)
- Tpe 1 1Document8 pagesTpe 1 1api-547598526100% (1)
- Methods of PhilosophizingDocument9 pagesMethods of PhilosophizingMikaella De Leon LayugNo ratings yet
- Project Two: Behavior Change BlueprintDocument4 pagesProject Two: Behavior Change BlueprintDevorah SanchezNo ratings yet
- Handouts Educ 202Document4 pagesHandouts Educ 202Lyza Rhane LapastoraNo ratings yet
- Iplan NoDocument4 pagesIplan NoHershaine PusodNo ratings yet
- Teacher's Book Project 1 PDFDocument1 pageTeacher's Book Project 1 PDFAldana SantarelliNo ratings yet
- Bring Your Favorite Countries To Life With Flags Coloring PagesDocument2 pagesBring Your Favorite Countries To Life With Flags Coloring PagesNabeel IsmailNo ratings yet
- Jebin Thomas Resume for MBA Graduate Seeking HR RoleDocument2 pagesJebin Thomas Resume for MBA Graduate Seeking HR Rolechunkz fever PRCNo ratings yet
- RRL ResearchDocument4 pagesRRL ResearchGlen Angela Mae PelayoNo ratings yet
- Mindsets:: How Beliefs Shape LearningDocument2 pagesMindsets:: How Beliefs Shape LearningHồ Thị Thùy Dung THCS&THPT U Minh Thượng - Kiên GiangNo ratings yet
- Quiz 2Document1 pageQuiz 2Dominga SarmientoNo ratings yet
- (BS ISO 12913-1 - 2014) - Acoustics. Soundscape. Definition and Conceptual Framework PDFDocument16 pages(BS ISO 12913-1 - 2014) - Acoustics. Soundscape. Definition and Conceptual Framework PDFwilson ardilaNo ratings yet
- PYC1501 Unit 1 Human Nervous System OERDocument18 pagesPYC1501 Unit 1 Human Nervous System OERjulia.mokoenadjNo ratings yet
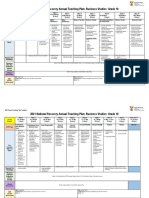
- 2023 Business Studies Grade 10 AtpDocument4 pages2023 Business Studies Grade 10 AtpKhozasuprise SandileNo ratings yet