You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Propranolol MueDocument12 pagesPropranolol Mueapi-535300613No ratings yet
- BurkhartbryceDocument24 pagesBurkhartbryceapi-535300613No ratings yet
- Burkhart CVDocument6 pagesBurkhart CVapi-535300613No ratings yet
- Cap Hap VapDocument2 pagesCap Hap Vapapi-535300613No ratings yet
- Psychosexual TheoryDocument27 pagesPsychosexual Theoryrejeneil100% (1)
- ASR-3000 Service ManualDocument26 pagesASR-3000 Service ManualYoussry Elsayed MohamedNo ratings yet
- Soal Ulangan Akhir SMTR 1 2019-2020 Bahasa Inggris Kelas 8Document4 pagesSoal Ulangan Akhir SMTR 1 2019-2020 Bahasa Inggris Kelas 8Esah El-NaseerNo ratings yet
- Miguel v. Montanez Case DigestDocument1 pageMiguel v. Montanez Case DigestMykee NavalNo ratings yet
- Posterior Crossbite in Primary and Mixed Dentition - Etiology and Management PedoDocument41 pagesPosterior Crossbite in Primary and Mixed Dentition - Etiology and Management PedoFourthMolar.comNo ratings yet
- Virgin Coconut OilDocument3 pagesVirgin Coconut OilEd CasasNo ratings yet
- The Central Pollution Control BoardDocument7 pagesThe Central Pollution Control BoardGanapati Joshi SankolliNo ratings yet
- Rosen 20kw Hybrid Kit - 7hours Self ConsumptionDocument1 pageRosen 20kw Hybrid Kit - 7hours Self Consumptiongihan_maNo ratings yet
- P2 Ped 030 ReviewerDocument6 pagesP2 Ped 030 ReviewerFrancis DeocaresNo ratings yet
- MorphineDocument3 pagesMorphineAizat KamalNo ratings yet
- Werner CH 4Document99 pagesWerner CH 4Osama NasimNo ratings yet
- Lennox Aqualean Awc Application Manual 32Document32 pagesLennox Aqualean Awc Application Manual 32André FerreiraNo ratings yet
- AC Rectifier Bulk Capacitor Selection With Analysis+SPICE (Walker) PDFDocument5 pagesAC Rectifier Bulk Capacitor Selection With Analysis+SPICE (Walker) PDFjazbo8No ratings yet
- Times Leader 06-04-2013Document32 pagesTimes Leader 06-04-2013The Times LeaderNo ratings yet
- MODULE in Stat Week 6Document10 pagesMODULE in Stat Week 6Joshua GonzalesNo ratings yet
- Improved Performance of EGR ValvesDocument2 pagesImproved Performance of EGR ValvesWilson BuenoNo ratings yet
- How To Read A Prescription Drug LabelDocument3 pagesHow To Read A Prescription Drug LabelJefriyanto Saud100% (2)
- CHAPTER LLDocument11 pagesCHAPTER LLDeege BaeNo ratings yet
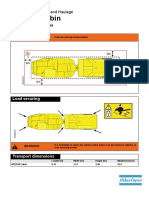
- 9852 2654 01 Transport Instructions MT2010 CabinDocument2 pages9852 2654 01 Transport Instructions MT2010 CabinIH Medrano100% (1)
- Science Quarter 1 Module 6Document44 pagesScience Quarter 1 Module 6shang121194% (32)
- SDS Carbon Coal ME50097Document10 pagesSDS Carbon Coal ME50097Stephen PerryNo ratings yet
- Inverter TrainerDocument2 pagesInverter TrainerBudhi PrasetiyoNo ratings yet
- Hearnshaw TSBE Conference Paper 2012Document8 pagesHearnshaw TSBE Conference Paper 2012FUCKUNo ratings yet
- Cojinete Teflon - GGB-HSG-High-Load-Fiber-Reinforced-Composite-PTFE-Bearing-DatasheetDocument2 pagesCojinete Teflon - GGB-HSG-High-Load-Fiber-Reinforced-Composite-PTFE-Bearing-DatasheetneodymioNo ratings yet
- Part3 Icho 11 15 PDFDocument124 pagesPart3 Icho 11 15 PDFManuel GuilhermeNo ratings yet
- Datasheet Nastra Uk 1.01 01Document1 pageDatasheet Nastra Uk 1.01 01Ahmed EbhaireNo ratings yet
- Schools of CriminologyDocument38 pagesSchools of Criminologykongthei100% (1)
- Sinamics G180: Converters - Compact Units, Cabinet Systems, Cabinet Units Air-Cooled and Liquid-CooledDocument240 pagesSinamics G180: Converters - Compact Units, Cabinet Systems, Cabinet Units Air-Cooled and Liquid-CooledAnonymous PDNToMmNmRNo ratings yet
- Cul5a - Lecture - Week 9 - Singaporean Cuisine PDFDocument14 pagesCul5a - Lecture - Week 9 - Singaporean Cuisine PDFJJ GRNo ratings yet
- Covenant On Civil and Political RightsDocument3 pagesCovenant On Civil and Political RightsRainier Rhett ConchaNo ratings yet