You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nursing Care PlanDocument4 pagesNursing Care Planmanu_gutierrez0891% (11)
- 2007, Vol.87, Issues 5, Vascular Surgery - New Concepts and Practice For The General SurgeonDocument320 pages2007, Vol.87, Issues 5, Vascular Surgery - New Concepts and Practice For The General SurgeonCitlalli Ortiz100% (1)
- Mizuho Vascular (Transcranial) DopplerDocument4 pagesMizuho Vascular (Transcranial) DopplersigmakarsaNo ratings yet
- The Endovascular Management of Ruptured Abdominal Aortic AneurysmsDocument12 pagesThe Endovascular Management of Ruptured Abdominal Aortic AneurysmsDiilNo ratings yet
- Case Study HypertensionDocument7 pagesCase Study Hypertensionsanthyakunjumon75% (4)
- Hemodynamic MonitoringDocument34 pagesHemodynamic Monitoringkurt94764No ratings yet
- Termodiluicao PulmonarDocument7 pagesTermodiluicao PulmonarKarina ResendeNo ratings yet
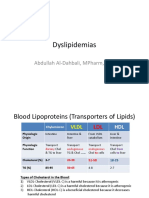
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 pagesDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- Cardiovascular WorksheetDocument4 pagesCardiovascular WorksheetAnonymous V7A9OKNo ratings yet
- A Study to Assess the Effectiveness of Video Assisted Teaching Module on Knowledge Regarding Myocardial Infarction and its Prevention among the Patients Attending Diabetic Clinic at BVV Sangha’s HSK Hospital and Research Centre, BagalkotDocument3 pagesA Study to Assess the Effectiveness of Video Assisted Teaching Module on Knowledge Regarding Myocardial Infarction and its Prevention among the Patients Attending Diabetic Clinic at BVV Sangha’s HSK Hospital and Research Centre, BagalkotInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nursing Care Plan For Pulmonary Edema PDFDocument2 pagesNursing Care Plan For Pulmonary Edema PDFAsmaa100% (1)
- Cardiac Musclet PDFDocument1 pageCardiac Musclet PDFمؤمل كامل عبد العالي هريسNo ratings yet
- Cartlidge Timothy Role of Percutaneous CoronaryDocument7 pagesCartlidge Timothy Role of Percutaneous Coronarybruno baileyNo ratings yet
- Circulatory System REVIEWERDocument6 pagesCirculatory System REVIEWERClyde BaltazarNo ratings yet
- Insufisiensi Vena Kronik: Akina Maulidhany Tahir, M.DDocument12 pagesInsufisiensi Vena Kronik: Akina Maulidhany Tahir, M.Dummu yayaNo ratings yet
- Worksheets-Respiratory and Circulatory SystemsDocument8 pagesWorksheets-Respiratory and Circulatory SystemsCarlos GuardadoNo ratings yet
- Principles of HemodynamicDocument48 pagesPrinciples of HemodynamicdevdsantoshNo ratings yet
- Patent Ductus ArteriosusDocument37 pagesPatent Ductus Arteriosuschiitoxin0% (1)
- Pathology of Renal Artery StenosisDocument24 pagesPathology of Renal Artery Stenosishamed8181No ratings yet
- 40-Article Text-54-1-10-20200920Document5 pages40-Article Text-54-1-10-20200920Alif Ibnu QoyyimNo ratings yet
- Anatomy of Esophagus and StomachDocument65 pagesAnatomy of Esophagus and Stomachmackiecc100% (2)
- Functions of The Muscular System IncludeDocument8 pagesFunctions of The Muscular System IncludeDanesh CamachoNo ratings yet
- Intracardiac PressuresDocument41 pagesIntracardiac Pressureswaleed315No ratings yet
- CALDOBDocument2 pagesCALDOBSatyendra Pandey50% (2)
- Duplex Ultrasound in The Diagnosis of Lower-Extremity DVTDocument5 pagesDuplex Ultrasound in The Diagnosis of Lower-Extremity DVTastraeax panda100% (1)
- Hemoptysis Revealing Intracardiac Thrombosis: A Case Report of Behcets DiseaseDocument5 pagesHemoptysis Revealing Intracardiac Thrombosis: A Case Report of Behcets DiseaseIJAR JOURNALNo ratings yet
- Blood Pressure ChartDocument4 pagesBlood Pressure ChartMelvyn Chavez MauricoNo ratings yet
- NNS Tutorial NotesDocument7 pagesNNS Tutorial NotesGio AmadorNo ratings yet
- Vascular AnastamosisDocument6 pagesVascular AnastamosissahandNo ratings yet
- Vitalsigns 180617200506Document34 pagesVitalsigns 180617200506Maricris Tac-an Calising-PallarNo ratings yet