You might also like
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Case StudyDocument49 pagesCase StudyLennie Marie B Pelaez100% (1)
- Ugib Case StudyDocument30 pagesUgib Case StudyVenus Glaze Verzola80% (5)
- Case Study Ugib Lower MBDocument65 pagesCase Study Ugib Lower MBQuolette Constante100% (1)
- NCP - Drug Study - Peptic UlcerDocument18 pagesNCP - Drug Study - Peptic UlcerEmi EspinoNo ratings yet
- Assessment Nursing Diagnosis Background Knowledge Planning Interventions Rationale Evaluation IndependentDocument5 pagesAssessment Nursing Diagnosis Background Knowledge Planning Interventions Rationale Evaluation IndependentLayne GazeNo ratings yet
- Case StudyDocument10 pagesCase StudyJib SinsuatNo ratings yet
- Upper Gastrointestinal BleedingDocument3 pagesUpper Gastrointestinal Bleedingplayaz_dan2100% (1)
- Case Study Ugib.Document19 pagesCase Study Ugib.Mary Ann Garcia100% (1)
- Colon Rectal CancerDocument6 pagesColon Rectal Cancerbryantmaroney811No ratings yet
- The Purpose of IV TherapyDocument5 pagesThe Purpose of IV TherapyBilly Ray Villanueva100% (1)
- Ov Ov OvDocument15 pagesOv Ov OvHayyana Mae Taguba LadiaNo ratings yet
- Breast Cancer Case StudyDocument5 pagesBreast Cancer Case StudyFrancesca ElixirNo ratings yet
- Ineffective Tissue Perfusion Secondary To Cellulitis DM Type 2Document3 pagesIneffective Tissue Perfusion Secondary To Cellulitis DM Type 2MichaelaKatrinaTrinidadNo ratings yet
- Gouty Arthritissss PathophyDocument2 pagesGouty Arthritissss Pathophybilliam123No ratings yet
- AcknowledgementDocument9 pagesAcknowledgementjhzenNo ratings yet
- AGE With Pa Tho PhysiologyDocument3 pagesAGE With Pa Tho PhysiologyChichi Licuben OresacamNo ratings yet
- NCP Fluid Volume DeficitDocument3 pagesNCP Fluid Volume DeficitNecheal BaayNo ratings yet
- Diverticular DiseaseDocument8 pagesDiverticular Diseasenurse_enzo100% (1)
- PathophysiologyDocument4 pagesPathophysiologyAngelou Joefred Congreso100% (1)
- Novilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationDocument1 pageNovilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationCharina AubreyNo ratings yet
- HYPERTENSION Health TeachingDocument3 pagesHYPERTENSION Health TeachingPaulo JavierNo ratings yet
- Discharge PlanDocument1 pageDischarge PlanBernalene SyNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationMara Jon Ocden CasibenNo ratings yet
- NCP2 - DengueDocument4 pagesNCP2 - DengueSummer SuarezNo ratings yet
- Age NCPDocument4 pagesAge NCPnj_pink081794No ratings yet
- Final Major Case StudyDocument17 pagesFinal Major Case Studyapi-546876878No ratings yet
- PATHOPHYSIOLOGYofDocument3 pagesPATHOPHYSIOLOGYofRose Si CheeksNo ratings yet
- NCP For UTIDocument3 pagesNCP For UTIlachrymoseai100% (4)
- Pa Tho Irritable Bowel SyndromeDocument1 pagePa Tho Irritable Bowel Syndromekaye0403No ratings yet
- Ugib Case StudyDocument36 pagesUgib Case StudyRJ MarquezNo ratings yet
- Leukemias: Care SettingDocument11 pagesLeukemias: Care SettingTinNo ratings yet
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsDocument4 pagesPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleNo ratings yet
- Case Presentation Hypokalemic ManDocument61 pagesCase Presentation Hypokalemic ManHussain AzharNo ratings yet
- Nephrolithiasis PDFDocument16 pagesNephrolithiasis PDFApriany Cordias Arlita SilalahiNo ratings yet
- Upper Gastrointestinal Bleeding: Anthony Alexander University of The West Indies at MonaDocument40 pagesUpper Gastrointestinal Bleeding: Anthony Alexander University of The West Indies at MonaAy Alex0% (1)
- CellulitisDocument12 pagesCellulitisAlma Bertos-Agub100% (1)
- CROHNSDocument2 pagesCROHNSAlvin Germo Pasuquin100% (1)
- General ObjectivesDocument1 pageGeneral ObjectivesErwin DegraciaNo ratings yet
- NCP Risk For InfectionDocument6 pagesNCP Risk For InfectionCazze SunioNo ratings yet
- Management and Prevention of Upper GI Bleeding: by Jiwon Kim, Pharm.D., BCPS, FCSHPDocument0 pagesManagement and Prevention of Upper GI Bleeding: by Jiwon Kim, Pharm.D., BCPS, FCSHPbasinang_jangil100% (1)
- Jose Rizal University & Medical Center: KardexDocument2 pagesJose Rizal University & Medical Center: KardexMichael SarmientoNo ratings yet
- Schistosomiasis (From Anatomy To Pathophysiology)Document10 pagesSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
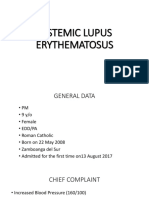
- Systemic Lupus ErythematosusDocument89 pagesSystemic Lupus ErythematosusIke RilleraNo ratings yet
- Case Liver CirrhosisDocument73 pagesCase Liver CirrhosisJesus Orita-Delima100% (1)
- Sle FinalDocument41 pagesSle FinalAsniah Hadjiadatu Abdullah100% (1)
- NCP DM and HCVDDocument3 pagesNCP DM and HCVDMAYBELINE OBAOB100% (1)
- Case Study On Fluid OverloadDocument37 pagesCase Study On Fluid OverloadradicalmpNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJanina Patricia BuddleNo ratings yet
- NCP DMDocument21 pagesNCP DMKate ManalastasNo ratings yet
- Pathophysiology of Atrial Septal DefectDocument2 pagesPathophysiology of Atrial Septal Defectbobtaguba50% (2)
- NCP Micu Hascvd Cad - RioDocument5 pagesNCP Micu Hascvd Cad - RioRio BonifacioNo ratings yet
- Ineffective Tissue Perfusion Related To Decrease Hemoglobin Concentration in The BloodDocument2 pagesIneffective Tissue Perfusion Related To Decrease Hemoglobin Concentration in The BloodKit Alizon BarredoNo ratings yet
- EndocrinedisorderDocument3 pagesEndocrinedisorderDyan LazoNo ratings yet
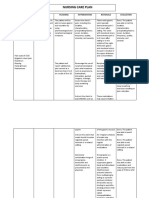
- Nursing Care PlanDocument7 pagesNursing Care PlanRhitzle Ann100% (1)
- Liver Case StudyDocument6 pagesLiver Case StudyGhulam MustafaNo ratings yet
- CHOLECYSTOLITHIASISDocument77 pagesCHOLECYSTOLITHIASISMarkie ArqueroNo ratings yet
- Gi-Rle - NCP For Deficient Fluid VolumeDocument2 pagesGi-Rle - NCP For Deficient Fluid VolumeEvangeline Villa de Gracia100% (1)
- Name: Wong Wai Kheong Matrix No: BMS12081154Document13 pagesName: Wong Wai Kheong Matrix No: BMS12081154myolie wuNo ratings yet
- IntussusceptionDocument27 pagesIntussusceptionimlookingforyou.03No ratings yet
- GIT Cirrhosis Liver in ChildrenDocument37 pagesGIT Cirrhosis Liver in ChildrenDr.P.NatarajanNo ratings yet
- Gastrointestinal DiseasesDocument853 pagesGastrointestinal DiseasesCiobanasu Denisa100% (1)
- Inflammatory Bowel Disease .. Last EditDocument22 pagesInflammatory Bowel Disease .. Last EditRashed ShatnawiNo ratings yet
- B3 Organisation and The Digestive System Exam-Style Answers: WWW - Oxfordsecondary.co - Uk/acknowledgementsDocument3 pagesB3 Organisation and The Digestive System Exam-Style Answers: WWW - Oxfordsecondary.co - Uk/acknowledgementsjimmy33% (3)
- ARLDDocument4 pagesARLDًNo ratings yet
- Accesories Advanced Endoscopy Olympus PDFDocument1 pageAccesories Advanced Endoscopy Olympus PDFJawia YusranNo ratings yet
- Cholelithiasis Case StudyDocument6 pagesCholelithiasis Case StudySarah DentyNo ratings yet
- Digestion and Absorption MCQsDocument3 pagesDigestion and Absorption MCQsSeekerNo ratings yet
- Bennett A Picture Guide of Chicken Feed WithdrawalDocument10 pagesBennett A Picture Guide of Chicken Feed Withdrawalachihaia100% (1)
- Points From Accupuncture AtlasDocument1 pagePoints From Accupuncture AtlasdishkuNo ratings yet
- Approach To Patients With Abdominal Pain-ValenDocument49 pagesApproach To Patients With Abdominal Pain-ValenCitra Sucipta0% (1)
- Pengaruh Terapi Dzikir Terhadap Intensitas Nyeri Pada Pasien GastritisDocument5 pagesPengaruh Terapi Dzikir Terhadap Intensitas Nyeri Pada Pasien GastritisFREDYANAK2 Istri1No ratings yet
- Cholestatic Liver Disease & Jaundice: Dr. David Minter, D.ODocument79 pagesCholestatic Liver Disease & Jaundice: Dr. David Minter, D.ONabeel ShahzadNo ratings yet
- 3 - Infectious DiarrheaDocument54 pages3 - Infectious DiarrheaTalha TariqNo ratings yet
- Laxatives AND Antidiarrheals: DR Mohd Suhaimi Jabatan FarmakologiDocument31 pagesLaxatives AND Antidiarrheals: DR Mohd Suhaimi Jabatan FarmakologiChokJunHoongNo ratings yet
- Feline AbdominAlDocument13 pagesFeline AbdominAlAlejandro Estrada RiosNo ratings yet
- Movicol Full DeckDocument107 pagesMovicol Full DeckMustafa JaradatNo ratings yet
- Ileus MeconiumDocument27 pagesIleus MeconiumDebby TamaraNo ratings yet
- Case Study 1 0 - Pancreatic Cancer FinalDocument23 pagesCase Study 1 0 - Pancreatic Cancer Finalapi-270737306No ratings yet
- Case StudyDocument21 pagesCase StudyFaye ingrid RasqueroNo ratings yet
- Small Intestinal Malabsorption in The Horse: An Assessment of The Specificity of The Oral Glucose Tolerance TestDocument3 pagesSmall Intestinal Malabsorption in The Horse: An Assessment of The Specificity of The Oral Glucose Tolerance Testdaniela betancurNo ratings yet
- UK Prof Hemorrhoids Piles Condition LeafletDocument6 pagesUK Prof Hemorrhoids Piles Condition Leafletmarisa apriliaNo ratings yet
- American Cancer SocietyDocument41 pagesAmerican Cancer SocietyEvi UtariNo ratings yet
- Arora PLAB 2 60 Day Planner - Min2Document9 pagesArora PLAB 2 60 Day Planner - Min2malmegrimNo ratings yet
- Colon Cancer 1 1Document30 pagesColon Cancer 1 1fall autumnNo ratings yet
- Biokimia 2 Sistem PencernaanDocument18 pagesBiokimia 2 Sistem PencernaanAnugrah NugraNo ratings yet
- Cholelithiasis in Children, Diagnosis and TreatmentDocument6 pagesCholelithiasis in Children, Diagnosis and TreatmentNur SulistiyaningsihNo ratings yet
- Motility Disorders of EsophagusDocument44 pagesMotility Disorders of EsophagusmackieccNo ratings yet
- Gastric CancerDocument31 pagesGastric CancerHarleen KaurNo ratings yet