You might also like
- Hyperthyroidism: Forms and Treatment OptionsDocument52 pagesHyperthyroidism: Forms and Treatment OptionsMedyWedhanggaNo ratings yet
- Hiper Dan Hipotiroid (Revisi)Document76 pagesHiper Dan Hipotiroid (Revisi)AgusNo ratings yet
- HipertiroidDocument48 pagesHipertiroidIlham KurniawanNo ratings yet
- Diseases of The ThyroidDocument65 pagesDiseases of The ThyroidEdil M JamaNo ratings yet
- Thyroid Disease: Sejal Nirban FY1Document30 pagesThyroid Disease: Sejal Nirban FY1Ahmed AbedoNo ratings yet
- Thyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistDocument30 pagesThyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistNurul HikmaNo ratings yet
- Mayuri Thyroid MTDocument24 pagesMayuri Thyroid MTmayuri zanwarNo ratings yet
- Thyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsDocument7 pagesThyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsPrincess Noreen SavellanoNo ratings yet
- SC2 2015 HyperthyroidismDocument38 pagesSC2 2015 HyperthyroidismShafern TanNo ratings yet
- Thyroiddisease 190216062020Document42 pagesThyroiddisease 190216062020Manikandan Vp100% (1)
- HipertiroidDocument31 pagesHipertiroidEdo Pramana PutraNo ratings yet
- HIPERTIROIDDocument30 pagesHIPERTIROIDNandaNo ratings yet
- ThyrotoxicosisDocument105 pagesThyrotoxicosisAli Murtaza Abbas100% (1)
- Thyroid Disease Guide: Symptoms, Diagnosis and TreatmentDocument32 pagesThyroid Disease Guide: Symptoms, Diagnosis and TreatmentAhmadAuliaFadlyRafNo ratings yet
- HipertiroidDocument37 pagesHipertiroidTaysqy swftNo ratings yet
- Endocrine System - Internal MedicineDocument39 pagesEndocrine System - Internal MedicineDaanishNo ratings yet
- Hi Per Tiro IdDocument46 pagesHi Per Tiro IdSri HazizahNo ratings yet
- Hyperthyroidism: Prevalence Women 2% Men 0.2% 15% of Cases Occur in Patients Older Than 60 Years of AgeDocument54 pagesHyperthyroidism: Prevalence Women 2% Men 0.2% 15% of Cases Occur in Patients Older Than 60 Years of AgeMegan MendozaNo ratings yet
- Kuliah HyperthyroidDocument18 pagesKuliah HyperthyroidFreddyNo ratings yet
- Mbs127 Slide Hyperthyroidism 1Document46 pagesMbs127 Slide Hyperthyroidism 1revita262No ratings yet
- Thyroid Gland Functions and Disorders ExplainedDocument35 pagesThyroid Gland Functions and Disorders ExplainedEdwin OkonNo ratings yet
- Plenary Week 1 LO No 1Document25 pagesPlenary Week 1 LO No 1Nur Faydotus SalsabilaNo ratings yet
- Unit II: Endocrine Nursing: Muhammad Yaqoob Instructor Ion-DuhsDocument51 pagesUnit II: Endocrine Nursing: Muhammad Yaqoob Instructor Ion-DuhsyaqoobmdNo ratings yet
- Thyroid Gland Diseases in ChildrenDocument29 pagesThyroid Gland Diseases in ChildrenadinayNo ratings yet
- Hyperthyroidism 1Document88 pagesHyperthyroidism 1Mamikie Vukeya100% (1)
- MerjohnDocument4 pagesMerjohnMerjohn LibutonNo ratings yet
- Thyrotoxicosis & Hypothyroidism by Prof DR NK ChopraDocument52 pagesThyrotoxicosis & Hypothyroidism by Prof DR NK ChopraAbdulsalam DostNo ratings yet
- HypertyroidismDocument46 pagesHypertyroidismenriNo ratings yet
- Gangguan Tiroid: - Elisabeth KasihDocument40 pagesGangguan Tiroid: - Elisabeth KasihFariza AndaniNo ratings yet
- Hyperthyroidism 1Document34 pagesHyperthyroidism 1mussavir100% (2)
- Thyroid DisordersDocument34 pagesThyroid DisordersAbdulhameed Mohamed100% (1)
- Thyroid DisorderDocument60 pagesThyroid DisorderThe AbyssinicansNo ratings yet
- Thyroiddisorders PDFDocument51 pagesThyroiddisorders PDFIslam ShoukryNo ratings yet
- Hypothyroidism: Autoimmune DiseaseDocument3 pagesHypothyroidism: Autoimmune DiseaseAnand SwamiNo ratings yet
- Thyroid Disorders ExplainedDocument28 pagesThyroid Disorders ExplainedMina RoxasNo ratings yet
- Hypothyroidism, Hyperthyroidism, Thyroid Nodules, and CancerDocument77 pagesHypothyroidism, Hyperthyroidism, Thyroid Nodules, and CancerDann San AntonioNo ratings yet
- Interpretation of Laboratory Thyroid Function Tests: The "Hidden" Health ProblemDocument38 pagesInterpretation of Laboratory Thyroid Function Tests: The "Hidden" Health Problemalanoud.877No ratings yet
- Thyroid Gland An Diseases of Thyroid D Gland: Omc LectureDocument59 pagesThyroid Gland An Diseases of Thyroid D Gland: Omc LectureEdward MakemboNo ratings yet
- Main Thyroid DiseasesDocument25 pagesMain Thyroid DiseasesPurnima ChoudhuryNo ratings yet
- Hyper and HypothyroidDocument139 pagesHyper and HypothyroidRaka ZaelaniNo ratings yet
- Hperthyroidism 1Document4 pagesHperthyroidism 1Salwa KaramanNo ratings yet
- HyperthyroidismDocument1 pageHyperthyroidismBeverly Bautista-OrtezaNo ratings yet
- Thyroid Disease: Apiradee SriwijitkamolDocument45 pagesThyroid Disease: Apiradee SriwijitkamolThorsang Chayovan50% (2)
- EndocrinologyDocument39 pagesEndocrinologySoumyajit Ray ChaudhuriNo ratings yet
- HyperthyroidismDocument23 pagesHyperthyroidism70 Kirithic Roshan RKNo ratings yet
- Thyroid Disorders Chapter 20 Hal 176 Dipiro Edisi 9Document7 pagesThyroid Disorders Chapter 20 Hal 176 Dipiro Edisi 9Nila LutfiNo ratings yet
- Thyroid Disease (Chan)Document29 pagesThyroid Disease (Chan)Sidiq AboobakerNo ratings yet
- Tyroid DiseasesDocument40 pagesTyroid DiseasesValentina MilovaNo ratings yet
- Endocrinology Board Review: Thyroid DisordersDocument46 pagesEndocrinology Board Review: Thyroid DisordersDemuel Dee L. BertoNo ratings yet
- Bening Disease of Thyroid GlandDocument85 pagesBening Disease of Thyroid GlandKarishma MishraNo ratings yet
- HyperthyroidismDocument4 pagesHyperthyroidismLamyaa Ali HasanNo ratings yet
- A CASE OF MULTINODULAR GOITREDocument27 pagesA CASE OF MULTINODULAR GOITREcnsatish86% (7)
- Hypothyroidism: Bagian Penyakit Dalam FK Uisu MedanDocument50 pagesHypothyroidism: Bagian Penyakit Dalam FK Uisu Medanindra saputraNo ratings yet
- Hyperthyroidism: ThyrotoxicosisDocument17 pagesHyperthyroidism: ThyrotoxicosisDerly Barino HasdiNo ratings yet
- Thyroid Function TestDocument21 pagesThyroid Function TestPat JacintoNo ratings yet
- Thyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoDocument35 pagesThyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoNinaNo ratings yet
- PEMERIKSAAAN LABORATORIUM KELAINAN THYROIDDocument12 pagesPEMERIKSAAAN LABORATORIUM KELAINAN THYROIDBonitavanyNo ratings yet
- Hypo and Hyperthyroidism 2023Document113 pagesHypo and Hyperthyroidism 2023Cristina Georgiana SerbanNo ratings yet
- HPERTHYROIDISMDocument4 pagesHPERTHYROIDISMSalwa KaramanNo ratings yet
- Development of Thyroid GlandDocument37 pagesDevelopment of Thyroid GlandnrahmaNo ratings yet
- Radiological Imaging of Ovarian Lesions.: Dr. Leni Santiana SP - RadDocument27 pagesRadiological Imaging of Ovarian Lesions.: Dr. Leni Santiana SP - RadnrahmaNo ratings yet
- Aging of The Endocrine SystemDocument23 pagesAging of The Endocrine SystemnrahmaNo ratings yet
- CSS - Advanced Life SupportDocument16 pagesCSS - Advanced Life SupportnrahmaNo ratings yet
- Iodine Deficiency Disorders: Diet S. Rustama R.M. Ryadi FadilDocument30 pagesIodine Deficiency Disorders: Diet S. Rustama R.M. Ryadi FadilnrahmaNo ratings yet
- Regulation of Calcium HomeostasisDocument11 pagesRegulation of Calcium HomeostasisnrahmaNo ratings yet
- Curriculum Vitae: Dr. Dr. Arto Yuwono Soeroto, SPPD-KP, FCCP, FinasimDocument62 pagesCurriculum Vitae: Dr. Dr. Arto Yuwono Soeroto, SPPD-KP, FCCP, FinasimnrahmaNo ratings yet
- Basic Life Support: Departemen Anestesiologi Dan Terapi Intensif Fakultas Kedokteran UNPAD / RSUP Hasan Sadikin BandungDocument32 pagesBasic Life Support: Departemen Anestesiologi Dan Terapi Intensif Fakultas Kedokteran UNPAD / RSUP Hasan Sadikin BandungnrahmaNo ratings yet
- Development of the Adrenal Glands (39 charactersDocument14 pagesDevelopment of the Adrenal Glands (39 charactersnrahmaNo ratings yet
- Mers-Cov ML PPSK Unpad 24 NovDocument33 pagesMers-Cov ML PPSK Unpad 24 NovnrahmaNo ratings yet
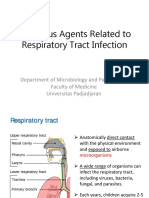
- The Role of Nutrition in Respiratory DiseaseDocument34 pagesThe Role of Nutrition in Respiratory DiseasenrahmaNo ratings yet
- Approach Pada Pasien DGN Kelainan TiroidDocument13 pagesApproach Pada Pasien DGN Kelainan TiroidnrahmaNo ratings yet
- Nuclear Medicine in Respiratory SystemDocument26 pagesNuclear Medicine in Respiratory SystemnrahmaNo ratings yet
- Asphyxial Death: Yoni SyukrianiDocument30 pagesAsphyxial Death: Yoni SyukrianinrahmaNo ratings yet
- Pulmonary Rehab: Comprehensive Team Approach for Chronic Lung DiseaseDocument29 pagesPulmonary Rehab: Comprehensive Team Approach for Chronic Lung DiseasenrahmaNo ratings yet
- Asphyxial Death: Yoni SyukrianiDocument30 pagesAsphyxial Death: Yoni SyukrianinrahmaNo ratings yet
- Skill Laboratory Practice Module Block: Neurobehavior and Special Sense System Topic: Developmental Reflexes General ObjectivesDocument4 pagesSkill Laboratory Practice Module Block: Neurobehavior and Special Sense System Topic: Developmental Reflexes General ObjectivesnrahmaNo ratings yet
- PULMONARY REHABILITATION-dr - Sunaryo BS, SPKFRDocument38 pagesPULMONARY REHABILITATION-dr - Sunaryo BS, SPKFRnrahmaNo ratings yet
- The Fungi of Medical ImportanceDocument74 pagesThe Fungi of Medical ImportancenrahmaNo ratings yet
- Ridad - One Health and ZoonosisDocument52 pagesRidad - One Health and ZoonosisnrahmaNo ratings yet
- Microbial Aspect of URTI MLDocument63 pagesMicrobial Aspect of URTI MLSherlyn YeeNo ratings yet
- Birth Trauma 1993Document8 pagesBirth Trauma 1993nrahmaNo ratings yet
- One Health: Tutor 2 FMDocument7 pagesOne Health: Tutor 2 FMnrahmaNo ratings yet
- One Health Core Competencies and Modules Presentation - Malaysia 8-10-17Document43 pagesOne Health Core Competencies and Modules Presentation - Malaysia 8-10-17nrahmaNo ratings yet
- Birth Injuries in Neonates 2016Document14 pagesBirth Injuries in Neonates 2016nrahmaNo ratings yet
- Bith Trauma Risk Factor & Short Term Outcome 2013Document5 pagesBith Trauma Risk Factor & Short Term Outcome 2013nrahmaNo ratings yet
- One Health: Tutor 2 FMDocument5 pagesOne Health: Tutor 2 FMnrahmaNo ratings yet
- Birth Injuries, Incidence, Perinatal Risk Factors & Outcomes - 2012Document8 pagesBirth Injuries, Incidence, Perinatal Risk Factors & Outcomes - 2012nrahmaNo ratings yet
- Birth Injuries: Causes, Presentation, and ManagementDocument4 pagesBirth Injuries: Causes, Presentation, and ManagementAngela Mitchelle NyanganNo ratings yet
- What Is Hashimoto's Disease?Document6 pagesWhat Is Hashimoto's Disease?Novia MentariNo ratings yet
- Exam 2 ReviewDocument31 pagesExam 2 ReviewAhsan Tebha50% (2)
- Thyroid Function Tests FaqDocument1 pageThyroid Function Tests FaqUttam AuddyNo ratings yet
- Mechanism of Action of Thyroid HormoneDocument4 pagesMechanism of Action of Thyroid HormonejaleelkabdulNo ratings yet
- David Perlmutter Focus Autoimmune PDFDocument23 pagesDavid Perlmutter Focus Autoimmune PDFutpal_thakar100% (6)
- HipotiroidDocument28 pagesHipotiroidmeongkorengNo ratings yet
- Endocrine Study GuideDocument4 pagesEndocrine Study GuideNursingSchoolNotes100% (1)
- HyperthyroidismDocument59 pagesHyperthyroidismjoanna73% (11)
- Thyroid Disorders TBL Pathology Learning MaterialDocument20 pagesThyroid Disorders TBL Pathology Learning MaterialIrdina SyabilNo ratings yet
- Hypertiroidismo Review Lancet 2022Document17 pagesHypertiroidismo Review Lancet 2022Diana Catalina Avila BareñoNo ratings yet
- Diabetes Mellietus: Types: PathogenesisDocument17 pagesDiabetes Mellietus: Types: PathogenesisSandip ChaudharyNo ratings yet
- Graves' Disease Signs and ManagementDocument11 pagesGraves' Disease Signs and ManagementManisha Sekaran Muniandy100% (1)
- Endocrinology - Internal Medicine, Dr. A. Mowafy (2020-2021)Document172 pagesEndocrinology - Internal Medicine, Dr. A. Mowafy (2020-2021)Mohammed RisqNo ratings yet
- Hypothyroidism 101: by Steven F. Hotze, M.DDocument31 pagesHypothyroidism 101: by Steven F. Hotze, M.DDewi SetyawatiNo ratings yet
- Standardized Lab Values - Final - 031215Document6 pagesStandardized Lab Values - Final - 031215isapatrick8126No ratings yet
- QuestionsDocument35 pagesQuestionsYasmeen AtiehNo ratings yet
- Excel Fro Payment LinkDocument7 pagesExcel Fro Payment LinkSanjay NadekarNo ratings yet
- Insert - Elecsys T3.ms - 11731360122.v26.enDocument4 pagesInsert - Elecsys T3.ms - 11731360122.v26.enGuneyden Guneyden100% (3)
- Fetuin-A Levels in Hyperthyroidism.Document5 pagesFetuin-A Levels in Hyperthyroidism.yekimaNo ratings yet
- Medicina 58 01115 v2Document21 pagesMedicina 58 01115 v2silmanuryanzila2705No ratings yet
- Thyroid in PregnancyDocument40 pagesThyroid in PregnancyGPFanNo ratings yet
- Merge-Davao (Multi - Educational Review Group Experts) : Physiological IntegrityDocument12 pagesMerge-Davao (Multi - Educational Review Group Experts) : Physiological IntegrityNom NomNo ratings yet
- ReportDocument2 pagesReportAnkita GoyalNo ratings yet
- Thyroid Hormone Synthesis, Hypothyroidism Causes, Signs, Diagnosis and TreatmentDocument15 pagesThyroid Hormone Synthesis, Hypothyroidism Causes, Signs, Diagnosis and TreatmentfachrulmirzaNo ratings yet
- Thyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. AvinashDocument9 pagesThyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. Avinashbelakang rumahNo ratings yet
- Thyroid Gland 2021Document28 pagesThyroid Gland 2021Dr. Ali100% (1)
- NeurotransmittersDocument4 pagesNeurotransmittersSalman Khan100% (1)
- 14 Foods Boost Your ThyroidDocument29 pages14 Foods Boost Your ThyroidDonciu Alexandra100% (1)
- Assessment of Thyroid FunctionDocument7 pagesAssessment of Thyroid FunctionDewi Paramita YuniarahmiNo ratings yet
- PASS - MRCOG Physiology 2017Document46 pagesPASS - MRCOG Physiology 2017reffyNo ratings yet