You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- ACS Biochemistry Study PrepDocument13 pagesACS Biochemistry Study PrepJOHN100% (2)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lakheri Cement Works: Report On Overhauling (Replacement of Internals) of Vrm-1 Main Gearbox 22-May-09 To 27-Jun-09Document47 pagesLakheri Cement Works: Report On Overhauling (Replacement of Internals) of Vrm-1 Main Gearbox 22-May-09 To 27-Jun-09sandesh100% (1)
- SyllabusDocument5 pagesSyllabusdvenumohanNo ratings yet
- Rehabilitation Guidelines For Total Hip (Anterior) ArthroplastyDocument4 pagesRehabilitation Guidelines For Total Hip (Anterior) ArthroplastydvenumohanNo ratings yet
- ICF-Ankle Trimalleolar FractureDocument18 pagesICF-Ankle Trimalleolar FracturedvenumohanNo ratings yet
- Sigma Medicare Systems: Quotation / Proforma InvoiceDocument17 pagesSigma Medicare Systems: Quotation / Proforma InvoicedvenumohanNo ratings yet
- Test-Retest Reliability and Validity of Three Different Agility Tests For Various Team Sports in Young Male AthletesDocument6 pagesTest-Retest Reliability and Validity of Three Different Agility Tests For Various Team Sports in Young Male AthletesdvenumohanNo ratings yet
- NDS Workshop OctDocument23 pagesNDS Workshop OctdvenumohanNo ratings yet
- Diwali: 28 October 2008 WALT Understand The Meaning of The Festival of DiwaliDocument11 pagesDiwali: 28 October 2008 WALT Understand The Meaning of The Festival of DiwalidvenumohanNo ratings yet
- Reliability of Clinical Tests To Evaluate Nerve Function and Mechanosensitivity of The Upper Limb Peripheral Nervous SystemDocument10 pagesReliability of Clinical Tests To Evaluate Nerve Function and Mechanosensitivity of The Upper Limb Peripheral Nervous SystemdvenumohanNo ratings yet
- Shortwave Diathermy: Prof. Dr. Gehan MosaadDocument29 pagesShortwave Diathermy: Prof. Dr. Gehan MosaaddvenumohanNo ratings yet
- Diwali the+Festival+of+LightsDocument12 pagesDiwali the+Festival+of+LightsdvenumohanNo ratings yet
- International College of Applied Kinesiology USA (PDFDrive)Document241 pagesInternational College of Applied Kinesiology USA (PDFDrive)dvenumohan100% (4)
- Z-Line Z-Line Actin Myosin: Na+ Na+ Na+ Na+ Na+ Na+Document35 pagesZ-Line Z-Line Actin Myosin: Na+ Na+ Na+ Na+ Na+ Na+dvenumohanNo ratings yet
- Total Hip Arthroplasty (THA) Rehabilitation ProtocolDocument11 pagesTotal Hip Arthroplasty (THA) Rehabilitation ProtocoldvenumohanNo ratings yet
- DigMandarin Grammar Lesson Comparison Sentence With Bi - 1 PDFDocument4 pagesDigMandarin Grammar Lesson Comparison Sentence With Bi - 1 PDFValentina BeltránNo ratings yet
- Oresome Handbook BCDDocument76 pagesOresome Handbook BCDlinmar7071No ratings yet
- New Almaz Rs KyyXXYGfXZDocument2 pagesNew Almaz Rs KyyXXYGfXZapriewanjudinNo ratings yet
- Quantum Physics NotesDocument1 pageQuantum Physics NotesChloe InnsNo ratings yet
- International Piano Competition R. Schumann - Fondazione CariptDocument2 pagesInternational Piano Competition R. Schumann - Fondazione Caripttoritori88No ratings yet
- Script Freebitco - in Strategy Calculator 2020Document5 pagesScript Freebitco - in Strategy Calculator 2020Netflix movies Watch and Download freeNo ratings yet
- Criminology The Essentials 3rd Edition Walsh Test Bank DownloadDocument35 pagesCriminology The Essentials 3rd Edition Walsh Test Bank DownloadJohn Adamson100% (26)
- MODULE 2 Analyzing Business TransactionsDocument18 pagesMODULE 2 Analyzing Business TransactionsKirk EscanillaNo ratings yet
- Resume SampleDocument1 pageResume SampleAnukrit AnilNo ratings yet
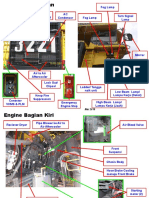
- KOMPONEN - HD785-7 SippDocument23 pagesKOMPONEN - HD785-7 Sippziky dun100% (1)
- J750 Basic Training Module1 J750 Tester OverviewDocument78 pagesJ750 Basic Training Module1 J750 Tester OverviewyohhongNo ratings yet
- Texapon SFA (OPP)Document1 pageTexapon SFA (OPP)paromanikNo ratings yet
- Theories of ManagementDocument46 pagesTheories of ManagementJanice FloridaNo ratings yet
- Tubos para Intercambiadores. Principales Medidas BWG.: ASTM Heat Exchanger Tube - Principal BWG SizesDocument1 pageTubos para Intercambiadores. Principales Medidas BWG.: ASTM Heat Exchanger Tube - Principal BWG SizesSaraMendozaNo ratings yet
- Cerruti RegisDocument18 pagesCerruti RegisNick MarkNo ratings yet
- 024 - Competence Requirements For Drilling and Well Service PersonnelDocument16 pages024 - Competence Requirements For Drilling and Well Service PersonnelmashanghNo ratings yet
- Phrasal VerbsDocument81 pagesPhrasal VerbsDien HamNo ratings yet
- PHDDocument215 pagesPHDCHIDINo ratings yet
- 1.3 Operating Systems: Ict IgcseDocument10 pages1.3 Operating Systems: Ict IgcseAqilah HasmawiNo ratings yet
- The New Companies Act (Chapter 24 - 31) Impact On Corporate Governance - Honey and BlanckenbergDocument5 pagesThe New Companies Act (Chapter 24 - 31) Impact On Corporate Governance - Honey and BlanckenbergLuke MadzikotoNo ratings yet
- Compulsory ExcessDocument2 pagesCompulsory ExcessAshok KumarNo ratings yet
- QSS TB ManualDocument63 pagesQSS TB Manualinno danNo ratings yet
- Product Development Training Module PDFDocument6 pagesProduct Development Training Module PDFMurshid IqbalNo ratings yet
- NetcraftDocument9 pagesNetcraftapi-238604507No ratings yet
- Control Component Easy: For VAV Terminal UnitsDocument36 pagesControl Component Easy: For VAV Terminal UnitssinisacarNo ratings yet
- Handbook3 VitaminA-1 PDFDocument5 pagesHandbook3 VitaminA-1 PDFJorge Luis RodríguezNo ratings yet
- CA Final Financial Reporting Self Study Notes by Ashwani JMLK3HFFDocument46 pagesCA Final Financial Reporting Self Study Notes by Ashwani JMLK3HFFJashwanthNo ratings yet
- Unit Plan English 9.4.2-DramaDocument5 pagesUnit Plan English 9.4.2-DramaMa.robelleF. Papa0% (1)