You might also like
- Power Breathe Plus English Plus ManualDocument8 pagesPower Breathe Plus English Plus ManualHerman Slokar Jr.No ratings yet
- Swiss Ball Enhances Lumbar Multifidus Activity in Chronic Low Back Pain 2015 Physical Therapy in SportDocument5 pagesSwiss Ball Enhances Lumbar Multifidus Activity in Chronic Low Back Pain 2015 Physical Therapy in SportJose J.No ratings yet
- PBS PrintDocument20 pagesPBS Printlisa ekaNo ratings yet
- Epicondylitis, Lateral: (Tennis Elbow)Document6 pagesEpicondylitis, Lateral: (Tennis Elbow)ArieZta Kautsar RahmanNo ratings yet
- Clinical Biomechanics of Gait: OutlineDocument7 pagesClinical Biomechanics of Gait: Outlinechacho1971100% (1)
- 7 NCPDocument7 pages7 NCPVina EmpialesNo ratings yet
- Lessonplan FinDocument14 pagesLessonplan Finx483xDNo ratings yet
- Lebanon Exams Mrcs Part A Sample QuestionsDocument6 pagesLebanon Exams Mrcs Part A Sample QuestionsNadir AlhussienyNo ratings yet
- Oxygenation Practice QuizDocument3 pagesOxygenation Practice QuizJoy Dunwan0% (1)
- Respiratory Diseases of NewbornDocument93 pagesRespiratory Diseases of NewbornTheva Thy100% (1)
- NRPDocument24 pagesNRPrajvikram8750% (6)
- Muscle Activation in Suspension TrainingDocument22 pagesMuscle Activation in Suspension TrainingRodrigo AlbuquerqueNo ratings yet
- Speed's test, biceps test, supraspinatus testsDocument8 pagesSpeed's test, biceps test, supraspinatus testsASM MutahirNo ratings yet
- Multifidus ExerciseDocument1 pageMultifidus ExerciseAna DuranNo ratings yet
- Coordination AssessmentDocument30 pagesCoordination AssessmentBhawna PalNo ratings yet
- AP41 MDocument3 pagesAP41 Monix2000No ratings yet
- BPPV and Lung Nodule GuideDocument4 pagesBPPV and Lung Nodule GuideKevin Roy MirandaNo ratings yet
- Physiotherapy management of paediatric flat feetDocument20 pagesPhysiotherapy management of paediatric flat feetCalvina Mizumi100% (1)
- Human Anatomy & PhysiologyDocument72 pagesHuman Anatomy & PhysiologyJoie UrsalNo ratings yet
- Vertigo and Its Management PDFDocument21 pagesVertigo and Its Management PDFNitya KrishnaNo ratings yet
- Stroke & Hemiplegia LocalizationDocument54 pagesStroke & Hemiplegia LocalizationVasu PottabatthiniNo ratings yet
- Vertigo Physiology and Clinical AssessmentDocument63 pagesVertigo Physiology and Clinical AssessmentdraseemmishraNo ratings yet
- Cutaneous Plantar SensorDocument5 pagesCutaneous Plantar Sensoronix2000No ratings yet
- Chapter # 4: Physical Assessment As A Screening ToolDocument89 pagesChapter # 4: Physical Assessment As A Screening Toolmuhammad awaisNo ratings yet
- The Brain Stem: Location and Basic PhysiologyDocument33 pagesThe Brain Stem: Location and Basic PhysiologyMohammad AliNo ratings yet
- Ataxias Neuro Condition DetailedDocument80 pagesAtaxias Neuro Condition DetailedMikail AtiyehNo ratings yet
- Craniovertebral Junction Anatomy & RadiologyDocument130 pagesCraniovertebral Junction Anatomy & Radiologydrarunrao100% (1)
- Congenital TorticollisDocument15 pagesCongenital TorticollisAryan WadhwaniNo ratings yet
- Pediatric Lower Extremity Orthopedic ConcernsDocument28 pagesPediatric Lower Extremity Orthopedic ConcernsDitaAnggaraKusumaNo ratings yet
- DR - Rieva Kuliah 7 November - 2018Document38 pagesDR - Rieva Kuliah 7 November - 2018Nisrina100% (1)
- Ankylosing Spondylitis Spine DiseaseDocument19 pagesAnkylosing Spondylitis Spine DiseaseZulhida YuniNo ratings yet
- Bells PalsyDocument66 pagesBells PalsyanshikaNo ratings yet
- Myopathies: Lecture ObjectivesDocument15 pagesMyopathies: Lecture ObjectivesanjelikaNo ratings yet
- Review of Literature PivdDocument5 pagesReview of Literature PivdPankaj VatsaNo ratings yet
- Hip Displacement in Cerebral PalsyDocument9 pagesHip Displacement in Cerebral PalsyJohannesSchoppmannNo ratings yet
- Acute Spinal Cord InjuryDocument3 pagesAcute Spinal Cord InjuryMarisol Dellera ValmoriaNo ratings yet
- Autonomic Nervous System: DR S S Ranasinghe CNTH - RagamaDocument63 pagesAutonomic Nervous System: DR S S Ranasinghe CNTH - RagamawellawalalasithNo ratings yet
- Vestibular Disorders and Rehab GuideDocument15 pagesVestibular Disorders and Rehab GuideMehul RathoreNo ratings yet
- Special Tests of The Hip & Pelvis: Kendall TestDocument5 pagesSpecial Tests of The Hip & Pelvis: Kendall Testsungmin kimNo ratings yet
- Cauda Equina and Conus Medullaris Syndromes Clinical PresentationDocument9 pagesCauda Equina and Conus Medullaris Syndromes Clinical PresentationhoneyworksNo ratings yet
- Pelvic Floor and Diaphragm Training for Core ProgramsDocument40 pagesPelvic Floor and Diaphragm Training for Core ProgramsGiritama IrwantoroNo ratings yet
- 9 Hip & Lumber DDDocument29 pages9 Hip & Lumber DDHeba Abo bakrNo ratings yet
- Spondylosis2 PDFDocument13 pagesSpondylosis2 PDFdrwarigitNo ratings yet
- Osteochondritis Dissecans: Vivek PandeyDocument25 pagesOsteochondritis Dissecans: Vivek PandeyRabin DasNo ratings yet
- Brachial Plexus InjuriesDocument64 pagesBrachial Plexus Injuriesprashanth naikNo ratings yet
- Congenital Muscular TorticollisDocument19 pagesCongenital Muscular TorticollisRyana AmazonaNo ratings yet
- Spina Bifida OCCULTADocument1 pageSpina Bifida OCCULTArebelswanteddot_comNo ratings yet
- Low Back Pain: Information For PatientsDocument0 pagesLow Back Pain: Information For PatientsRavisankar PeriasamyNo ratings yet
- What To Expect With Spina Bifida Occulta: Find Support For Your Mental HealthDocument2 pagesWhat To Expect With Spina Bifida Occulta: Find Support For Your Mental Healthmiftah8885No ratings yet
- Managing LymphedemaDocument8 pagesManaging Lymphedemaوحش الصاعقهNo ratings yet
- Deep Cervical Fascia by Talha JavedDocument45 pagesDeep Cervical Fascia by Talha JavedTalha Javed100% (1)
- Proprioception 2009Document32 pagesProprioception 2009deleted1610100% (2)
- PostureDocument2 pagesPostureNader MorrisNo ratings yet
- Sciatica3 MBW 20110922 PDFDocument5 pagesSciatica3 MBW 20110922 PDFTrandafir LacramioaraNo ratings yet
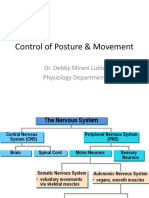
- Control of Posture & Movement-Blok15Document36 pagesControl of Posture & Movement-Blok15BonitavanyNo ratings yet
- Amputation - Gait Deviations: Analysis of Transtibial (Below-Knee) Amputee GaitDocument9 pagesAmputation - Gait Deviations: Analysis of Transtibial (Below-Knee) Amputee GaitArchana MohantyNo ratings yet
- Cerebellar Stroke Causes, Symptoms & TreatmentDocument17 pagesCerebellar Stroke Causes, Symptoms & TreatmentAna CotomanNo ratings yet
- Deep Tendon Reflex Examination GuideDocument4 pagesDeep Tendon Reflex Examination GuideDan Ali100% (1)
- Pelvic Fractures - These Can Kill YouDocument20 pagesPelvic Fractures - These Can Kill YouSurgicalgownNo ratings yet
- Spine Emergencies: Spinal Cord Injury (SCI) - The BasicsDocument67 pagesSpine Emergencies: Spinal Cord Injury (SCI) - The Basicsditya_madridistasNo ratings yet
- Degenerative Joint Diseases - Admisson ExamDocument23 pagesDegenerative Joint Diseases - Admisson ExamNona NadimNo ratings yet
- Rotator Cuff Assessment PDFDocument11 pagesRotator Cuff Assessment PDFMichele MarengoNo ratings yet
- Seminar On Gait Rehab in PDDocument41 pagesSeminar On Gait Rehab in PDPriya KuberanNo ratings yet
- Endocrine Response Ni FinalDocument35 pagesEndocrine Response Ni FinalSaktriawan ArifNo ratings yet
- VertigoDocument50 pagesVertigosaltoftheearthlightoftheworld506No ratings yet
- Regional Nerve Blocks And Infiltration Therapy: Textbook and Color AtlasFrom EverandRegional Nerve Blocks And Infiltration Therapy: Textbook and Color AtlasDanilo JankovicNo ratings yet
- Balance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementFrom EverandBalance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementNo ratings yet
- TB Peritonitis Diagnosis and TreatmentDocument9 pagesTB Peritonitis Diagnosis and TreatmentashuNo ratings yet
- Getahun Mengistu, MD, MSC, Internist, Neurologist & Specialist in Headache Medicine, Department of Neurology, AAU-MFDocument85 pagesGetahun Mengistu, MD, MSC, Internist, Neurologist & Specialist in Headache Medicine, Department of Neurology, AAU-MFashuNo ratings yet
- Seisure Disorder: by Abebe DendirDocument52 pagesSeisure Disorder: by Abebe DendirashuNo ratings yet
- Respiratory System: Physical Diagnosis Course II Physical ExamDocument57 pagesRespiratory System: Physical Diagnosis Course II Physical ExamashuNo ratings yet
- Lymphoproliferative Disorders: Chronic Lymphocytic Leukemia-CLL Hairy Cell Leukemia Plasma Cell DisordersDocument42 pagesLymphoproliferative Disorders: Chronic Lymphocytic Leukemia-CLL Hairy Cell Leukemia Plasma Cell DisordersyosefNo ratings yet
- Neurologic ExaminationDocument4 pagesNeurologic ExaminationashuNo ratings yet
- Managing Opportunistic Malignancies in HIV PatientsDocument23 pagesManaging Opportunistic Malignancies in HIV PatientsashuNo ratings yet
- Approach to Coma: Assessment, Management and PrognosisDocument36 pagesApproach to Coma: Assessment, Management and PrognosisashuNo ratings yet
- Childhood Seizure DisordersDocument57 pagesChildhood Seizure DisordersashuNo ratings yet
- Acute LeukemiaDocument43 pagesAcute LeukemiaashuNo ratings yet
- AFI Lecture UGDocument55 pagesAFI Lecture UGashuNo ratings yet
- Approach To Comatose Patient: Abyot B5 Female SideDocument16 pagesApproach To Comatose Patient: Abyot B5 Female SideashuNo ratings yet
- Pulmonary Manifestations of HIVDocument11 pagesPulmonary Manifestations of HIVashuNo ratings yet
- Gastrointestinal Manifestation of HIVDocument16 pagesGastrointestinal Manifestation of HIVashuNo ratings yet
- Acute Febrile Illnesses ManagementDocument124 pagesAcute Febrile Illnesses ManagementashuNo ratings yet
- Skin Manifestations of HIVDocument11 pagesSkin Manifestations of HIVashuNo ratings yet
- AmebiasisDocument34 pagesAmebiasisashuNo ratings yet
- Skin Manifestations of HIVDocument11 pagesSkin Manifestations of HIVashuNo ratings yet
- ComaDocument18 pagesComaashuNo ratings yet
- Neurologic ExaminationDocument4 pagesNeurologic ExaminationashuNo ratings yet
- Gastrointestinal Manifestation of HIVDocument16 pagesGastrointestinal Manifestation of HIVashuNo ratings yet
- Immune Reconstitution Inflammatory Syndrome (Iris)Document6 pagesImmune Reconstitution Inflammatory Syndrome (Iris)ashuNo ratings yet
- Acute Febrile Illnesses ManagementDocument124 pagesAcute Febrile Illnesses ManagementashuNo ratings yet
- Pulmonary Manifestations of HIVDocument11 pagesPulmonary Manifestations of HIVashuNo ratings yet
- AmebiasisDocument34 pagesAmebiasisashuNo ratings yet
- Childhood Seizure DisordersDocument57 pagesChildhood Seizure DisordersashuNo ratings yet
- TB Peritonitis Diagnosis and TreatmentDocument9 pagesTB Peritonitis Diagnosis and TreatmentashuNo ratings yet
- ComaDocument18 pagesComaashuNo ratings yet
- Acute LeukemiaDocument43 pagesAcute LeukemiaashuNo ratings yet
- Physical Examination in Respiratory SystemDocument58 pagesPhysical Examination in Respiratory SystemMarian0% (1)
- Estudio Drenajes ToracicosDocument8 pagesEstudio Drenajes Toracicosyaizagcasado26No ratings yet
- Post Tubercular Sequelae.123175034Document29 pagesPost Tubercular Sequelae.123175034Andre Prasetyo MahesyaNo ratings yet
- Peripheral, Head and Neck Surgery: Brendon J. Coventry EditorDocument167 pagesPeripheral, Head and Neck Surgery: Brendon J. Coventry EditorMariaNo ratings yet
- 5 Patient Assessment Skills To Crush The TMC-RRT ExamDocument4 pages5 Patient Assessment Skills To Crush The TMC-RRT ExamNaser Abdulfatah Al Hazmi100% (1)
- Caring For Patients With Chest Tubes PDFDocument10 pagesCaring For Patients With Chest Tubes PDFSavanna ChambersNo ratings yet
- Tension Pneumothorax in A Patient With COVID-19Document4 pagesTension Pneumothorax in A Patient With COVID-19InggitNo ratings yet
- Physiology of the Pleural Space: Visceral Pleura, Parietal Pleura, and Fluid FormationDocument78 pagesPhysiology of the Pleural Space: Visceral Pleura, Parietal Pleura, and Fluid FormationAhmad RafiqiNo ratings yet
- V.I. Vernadsky Crimean Federal University Medical Academy named after S.I. Georgievsky Chair of Surgery No1 Objectives for Intermediate Certification 6 yearDocument49 pagesV.I. Vernadsky Crimean Federal University Medical Academy named after S.I. Georgievsky Chair of Surgery No1 Objectives for Intermediate Certification 6 yearjhuiNo ratings yet
- Chest TraumaDocument52 pagesChest TraumaSllavko K. KallfaNo ratings yet
- Manajemen Trauma ThoraksDocument62 pagesManajemen Trauma ThoraksqweqweqwNo ratings yet
- Clinical Ultrasound A How-To GuideDocument146 pagesClinical Ultrasound A How-To GuideNacko Stavreski67% (3)
- Nursing Management of Patients WithDocument8 pagesNursing Management of Patients Withfunky goodNo ratings yet
- Surgical and Medical Emergencies UpDocument80 pagesSurgical and Medical Emergencies Upyvettefankam82No ratings yet
- Chest Trauma FinalDocument20 pagesChest Trauma FinalJem TellainNo ratings yet
- Pleural Effusion Causes and DiagnosisDocument69 pagesPleural Effusion Causes and DiagnosisUswatun Hasanah RINo ratings yet
- Thoracic Pathology: Dr. Fatima Ejaz PT Ms Neuro Physical TherapyDocument24 pagesThoracic Pathology: Dr. Fatima Ejaz PT Ms Neuro Physical Therapykim suhoNo ratings yet
- TV MCQ Pertanyaan TokDocument5 pagesTV MCQ Pertanyaan TokdhinahafizNo ratings yet
- Activity 3Document7 pagesActivity 3Naditha Putri HandayaniNo ratings yet
- NCM 103 Final ExamDocument13 pagesNCM 103 Final Examd1choosen100% (1)
- International Journal of Surgery Case ReportsDocument3 pagesInternational Journal of Surgery Case Reportssiska khairNo ratings yet
- Updated Writing Case Notes With SamplesDocument16 pagesUpdated Writing Case Notes With Samplessunil wesley100% (8)
- JRNL-Responding To Trauma Your Priorities in The First HourDocument8 pagesJRNL-Responding To Trauma Your Priorities in The First HourArs MoriendiNo ratings yet