You might also like
- Physiology of MenstrationDocument33 pagesPhysiology of MenstrationYiel Ellie Balase Moldin100% (1)
- CONTRACEPTION LectureDocument49 pagesCONTRACEPTION LectureAnton OcampoNo ratings yet
- High Risk PregnancyDocument113 pagesHigh Risk PregnancyVivian Lajara100% (2)
- Placenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaDocument72 pagesPlacenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaEsa SthaNo ratings yet
- The Premature BabyDocument92 pagesThe Premature BabyTrishenth Fonseka100% (1)
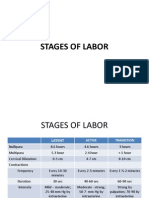
- Stages of LaborDocument30 pagesStages of LaborPerrilyn Perey100% (1)
- Polycystic Ovarian SyndromeDocument47 pagesPolycystic Ovarian SyndromeAnonymous HgX3mN1o100% (1)
- Reproduction Concept MapDocument1 pageReproduction Concept Mapapi-392216729No ratings yet
- Physiological Changes in Pregnancy PresentationDocument9 pagesPhysiological Changes in Pregnancy PresentationAyazNo ratings yet
- High Risk PregnancyDocument12 pagesHigh Risk Pregnancyggrrk7100% (2)
- Fertilization &implantationDocument30 pagesFertilization &implantationAzza100% (1)
- Patient's Bill of Rights (Philippines)Document16 pagesPatient's Bill of Rights (Philippines)KarlaBadongNo ratings yet
- Physiologic and Psychologic Changes in PregnancyDocument41 pagesPhysiologic and Psychologic Changes in PregnancyAlessandra Franchesca CortezNo ratings yet
- DM in PregnancyDocument35 pagesDM in Pregnancyapule geraldhumbleNo ratings yet
- Menstrual Cycle Lecture NotesDocument23 pagesMenstrual Cycle Lecture Notespmkobar461250% (2)
- Chapter 10 Physiological Psychological Changes in PregnancyDocument48 pagesChapter 10 Physiological Psychological Changes in PregnancyJeremiah Paul Gotia Humiwat100% (2)
- Artificial InseminationDocument41 pagesArtificial Inseminationsubalini100% (1)
- Ethical Issues in Assisted ReproductionDocument38 pagesEthical Issues in Assisted ReproductionAdaiah Priscillia SoibiharryNo ratings yet
- Physical Examination For Pregnant WomanDocument31 pagesPhysical Examination For Pregnant WomanFrancia ToledanoNo ratings yet
- Definition of InfertilityDocument6 pagesDefinition of InfertilityRatiram LilhareNo ratings yet
- Contraception: DR Husni SamarahDocument15 pagesContraception: DR Husni Samarahpal_pal_palNo ratings yet
- Abruptio Placenta and AbortionDocument10 pagesAbruptio Placenta and Abortiondanica grace gubaNo ratings yet
- Female Reproductive AnatomyDocument28 pagesFemale Reproductive AnatomySuho Leexokleader KimNo ratings yet
- GonorrheaDocument4 pagesGonorrheaNader Smadi100% (1)
- Colostomy CareDocument34 pagesColostomy CareTolemre EmreNo ratings yet
- Anatomy and Physiology of Female Reproductive System 1Document3 pagesAnatomy and Physiology of Female Reproductive System 1gilbertgarciaNo ratings yet
- 1Document11 pages1Mart AlunanNo ratings yet
- Fertilization & ImplantationDocument61 pagesFertilization & ImplantationchidimmaNo ratings yet
- 22 Cephalo-Pelvic DisproportionDocument32 pages22 Cephalo-Pelvic DisproportionNirupama KsNo ratings yet
- Dr. Ravichandran Doraiswamy Professor of AnatomyDocument70 pagesDr. Ravichandran Doraiswamy Professor of AnatomySiva SrinivasanNo ratings yet
- Multiple PregnancyDocument55 pagesMultiple PregnancyNathaniel YeriNo ratings yet
- Abnormal Labor and DeliveryDocument56 pagesAbnormal Labor and Deliveryanon_55864979No ratings yet
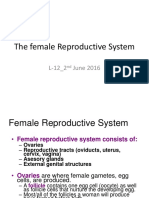
- The Female Reproductive System AutosavedDocument49 pagesThe Female Reproductive System AutosavedVenice izza Venancio100% (1)
- Gram Positive and Gram NegativeDocument3 pagesGram Positive and Gram NegativeMaclord GolvinNo ratings yet
- Reproductive EndocrinologyDocument18 pagesReproductive EndocrinologyAnonymous hkWIKjoXFVNo ratings yet
- Assisted Reproductive TechniquesDocument10 pagesAssisted Reproductive TechniquesSubhangi Lenka50% (2)
- From Egg and Sperm To NewbornDocument63 pagesFrom Egg and Sperm To NewbornCristine Joy GuinoNo ratings yet
- Chapter 9 - Drug Therapy During PregnancyDocument3 pagesChapter 9 - Drug Therapy During Pregnancydlneisha61No ratings yet
- Case StudyDocument48 pagesCase Studysimbarashe tangwadzanaNo ratings yet
- Complications of PregnancyDocument33 pagesComplications of PregnancyMilagros Maglasang100% (1)
- ABORTIONDocument23 pagesABORTIONCristyl Shine BariaoNo ratings yet
- What Is RH IncompatibilityDocument22 pagesWhat Is RH IncompatibilityKimsha ConcepcionNo ratings yet
- InfertilityDocument10 pagesInfertilityits_piks7256No ratings yet
- 52 Lecture The Diagnosis of PregnancyDocument75 pages52 Lecture The Diagnosis of PregnancyTarek TarekNo ratings yet
- Hiv Infection in PregnancyDocument19 pagesHiv Infection in PregnancyFathima NazarNo ratings yet
- FERTILIZATIONDocument180 pagesFERTILIZATIONPaul Kevin Mendoza67% (3)
- Seminar On InfertilityDocument17 pagesSeminar On InfertilityN vineethaNo ratings yet
- FAMILY PLANNING PROGRAM HandoutsDocument2 pagesFAMILY PLANNING PROGRAM HandoutsWilma Nierva BeraldeNo ratings yet
- MCSP Kenya Complementary Feeding Recipe BookletDocument28 pagesMCSP Kenya Complementary Feeding Recipe BookletAfifa Prima GittaNo ratings yet
- Normal Menstrual CycleDocument20 pagesNormal Menstrual CycleTrevor UratelNo ratings yet
- Menstrual CycleDocument11 pagesMenstrual CycleNP100% (1)
- Physiology of Normal' LabourDocument23 pagesPhysiology of Normal' LabourPrabhakar Kumar100% (2)
- Menstrual CycleDocument11 pagesMenstrual CycleSteph QuisquinoNo ratings yet
- Reproductive and Sexual Health NotesDocument9 pagesReproductive and Sexual Health NotesKayeNo ratings yet
- High Risk PregnancyDocument14 pagesHigh Risk PregnancyJezrael PueblosNo ratings yet
- Mechanism of Labor: Presented By: GROUP 1Document11 pagesMechanism of Labor: Presented By: GROUP 1Mary Christine Estrada Cabactulan100% (1)
- Induction and Augmentation of Labor (v2)Document49 pagesInduction and Augmentation of Labor (v2)Mara Medina - BorleoNo ratings yet
- Accessory OrgansDocument43 pagesAccessory Organslouradel100% (1)
- Nursing-Interventions MCN For Infertility MenDocument2 pagesNursing-Interventions MCN For Infertility MenRio DanteNo ratings yet
- Diagnosis of PregnancyDocument42 pagesDiagnosis of PregnancyAastha BistaNo ratings yet
- DX of PregnancyDocument41 pagesDX of Pregnancyshivamg.sg1234No ratings yet
- Processing of The Skills Laboratory Activity: Obstetric History Determining The GTPAL, EDD and AOGDocument26 pagesProcessing of The Skills Laboratory Activity: Obstetric History Determining The GTPAL, EDD and AOGFrancr ToledanoNo ratings yet
- Collection of SpecimenDocument21 pagesCollection of SpecimenFrancr ToledanoNo ratings yet
- Care of The Woman During PregnancyDocument99 pagesCare of The Woman During PregnancyFrancr ToledanoNo ratings yet
- Medical and Surgical AsepsisDocument40 pagesMedical and Surgical AsepsisFrancr ToledanoNo ratings yet
- Initial Care of BurnsDocument53 pagesInitial Care of BurnsFrancr ToledanoNo ratings yet
- Acute CareDocument50 pagesAcute CareFrancr ToledanoNo ratings yet
- Injuries To MSKDocument25 pagesInjuries To MSKFrancr ToledanoNo ratings yet
- Intravenous TherapyDocument48 pagesIntravenous TherapyFrancr ToledanoNo ratings yet
- Classification/staging Systems For Endometriosis: The State of The ArtDocument9 pagesClassification/staging Systems For Endometriosis: The State of The ArtMerlin MuktialiNo ratings yet
- GynatresiaDocument24 pagesGynatresiaapi-3705046100% (6)
- Vaginal Breech DeliveryDocument33 pagesVaginal Breech DeliveryTriani Dwi NingsihNo ratings yet
- Management of Abnormal Uterine Bleeding - UpToDateDocument25 pagesManagement of Abnormal Uterine Bleeding - UpToDatePollyannaLimadeCastroNo ratings yet
- The Female Reproductive SystemDocument22 pagesThe Female Reproductive SystemAnisatul Khabibah ZaenNo ratings yet
- Empanelled Hospitals CGHSDocument107 pagesEmpanelled Hospitals CGHSankit.shrivastavaNo ratings yet
- Fibroid Uterus 2019Document60 pagesFibroid Uterus 2019Mahmoud Abu Al AmrainNo ratings yet
- Sopk FezolinetantDocument43 pagesSopk FezolinetantOurroz DurandikNo ratings yet
- Addressing Needs For Fistula Training in Subsaharan AfricaDocument63 pagesAddressing Needs For Fistula Training in Subsaharan Africaapeksha500No ratings yet
- SSG 1 (Reproductive Development)Document5 pagesSSG 1 (Reproductive Development)Kaye Zelen LautaNo ratings yet
- Reproductive Models LabeledDocument15 pagesReproductive Models LabeledBao LinhNo ratings yet
- Menstrual Disorders DefinitionDocument4 pagesMenstrual Disorders DefinitionabraryeniNo ratings yet
- An Anatomico Clinical Study of Artav Vaha Srotas W.S.R. To DysmenorrhoeaDocument5 pagesAn Anatomico Clinical Study of Artav Vaha Srotas W.S.R. To DysmenorrhoeaEditor IJTSRDNo ratings yet
- FSRH Guidance: Switching or Starting Methods of ContraceptionDocument11 pagesFSRH Guidance: Switching or Starting Methods of ContraceptionNik NurwaniNo ratings yet
- Your Complete Guide To Birth Control Methods in The PhilippinesDocument8 pagesYour Complete Guide To Birth Control Methods in The PhilippinesJobert John BatallonesNo ratings yet
- 陳v Endometrial Cancer 2Document48 pages陳v Endometrial Cancer 201范芷紜No ratings yet
- Assessment of The Female Genitalia and RectumDocument2 pagesAssessment of The Female Genitalia and RectumLi mNo ratings yet
- Family Planning (Responsible Parenthood and Birth Control)Document14 pagesFamily Planning (Responsible Parenthood and Birth Control)Kirt Jean Cael50% (2)
- Hormonal Imbalance and Its Causes in Young Females: January 2015Document6 pagesHormonal Imbalance and Its Causes in Young Females: January 2015figgernaggotNo ratings yet
- Assisted Reproductive TechnologyDocument28 pagesAssisted Reproductive TechnologyftvyvyvNo ratings yet
- Postnatal PalpationDocument21 pagesPostnatal PalpationAnonymous 4txA8N8etNo ratings yet
- Abortion TypesDocument19 pagesAbortion TypesFany MaldoNo ratings yet
- Premature Cervical DilatationDocument3 pagesPremature Cervical DilatationEllaNo ratings yet
- IIII :::: : S EsentDocument22 pagesIIII :::: : S EsentCharlie AbagonNo ratings yet
- Dilation and Curettage Janelle ReforDocument4 pagesDilation and Curettage Janelle ReforCjay HernandezNo ratings yet
- Lesson 4 Biomedical Perspective in Gender Sexuality 2Document28 pagesLesson 4 Biomedical Perspective in Gender Sexuality 2Nikka GoenettNo ratings yet
- Genital Prolapse and HomoeopathyDocument69 pagesGenital Prolapse and HomoeopathyAnmol AgrawalNo ratings yet
- Chari. - For MergeDocument6 pagesChari. - For MergeMark ElbenNo ratings yet
- Puberty Is The Time When Our Body Changes PhysicallyDocument3 pagesPuberty Is The Time When Our Body Changes PhysicallyDemelzå SasotaNo ratings yet