You might also like
- The Risks Of Alcohol During Pregnancy - Based On The Teachings Of Dr. Andrew Huberman: Safeguarding MotherhoodFrom EverandThe Risks Of Alcohol During Pregnancy - Based On The Teachings Of Dr. Andrew Huberman: Safeguarding MotherhoodNo ratings yet
- MCN Finals NotesDocument495 pagesMCN Finals NotesLeigh JiandNo ratings yet
- HIGH RISK PREGNANCY (Bleeding Disorders) PDFDocument65 pagesHIGH RISK PREGNANCY (Bleeding Disorders) PDFAthena Dela CruzNo ratings yet
- Newborn ConditionsDocument80 pagesNewborn ConditionsrigasanaorayNo ratings yet
- High Risk Pregnancy: Alliah Claire Carnice BaguioDocument3 pagesHigh Risk Pregnancy: Alliah Claire Carnice BaguiokirbsNo ratings yet
- High Risk Newborn ModuleDocument6 pagesHigh Risk Newborn ModuleRastie MendozaNo ratings yet
- High Risk Pregnancy NCM 109Document2 pagesHigh Risk Pregnancy NCM 109TechnoShindoNo ratings yet
- Detty S2 Gizi Nutrition PreconceptionDocument25 pagesDetty S2 Gizi Nutrition PreconceptionyuniarsyNo ratings yet
- Cornell's Note 4Document5 pagesCornell's Note 4Angel BriboneriaNo ratings yet
- Fetal DistressDocument3 pagesFetal DistressMaria Donabella OngueNo ratings yet
- Usg Webinar Bioprofil Bayi PrintDocument36 pagesUsg Webinar Bioprofil Bayi PrintElfan WinotoNo ratings yet
- HANDOUTDocument10 pagesHANDOUTMerly Grael LigligenNo ratings yet
- What Should You KnowDocument2 pagesWhat Should You KnowCeline PanahonNo ratings yet
- Concepts in Public He Alth: A Case Study of Protein Energy Malnutrition (PEM)Document21 pagesConcepts in Public He Alth: A Case Study of Protein Energy Malnutrition (PEM)Aswin AshNo ratings yet
- D. High Risk PregnanciesDocument78 pagesD. High Risk PregnanciesKeziah TampusNo ratings yet
- Assessment of High-Risk PregnancyDocument23 pagesAssessment of High-Risk PregnancyNiña Ricci MtflcoNo ratings yet
- Obstetric BleedingDocument1 pageObstetric BleedingZiyadNo ratings yet
- Intrauterine Growth Restriction (IUGR)Document29 pagesIntrauterine Growth Restriction (IUGR)Lana LocoNo ratings yet
- Maternal and Child Health Nursing L E C T U R EDocument12 pagesMaternal and Child Health Nursing L E C T U R EAngelica Dalit MendozaNo ratings yet
- Malnutriția: Dr. Oana Falup 2017-2018Document86 pagesMalnutriția: Dr. Oana Falup 2017-2018Alina CamerzanNo ratings yet
- Maternal 2 Lecture All Lessons 2Document29 pagesMaternal 2 Lecture All Lessons 2Julian SantosNo ratings yet
- Vigilancia Fetal Anteparto Con ComentariosDocument72 pagesVigilancia Fetal Anteparto Con ComentariosEsme Tecuanhuehue PaulinoNo ratings yet
- Complication On Labor and DeliveryDocument5 pagesComplication On Labor and DeliveryMeryville JacildoNo ratings yet
- Module No. Date: Topic:: Cues/Questions/Keywords NotesDocument103 pagesModule No. Date: Topic:: Cues/Questions/Keywords Notesanon ymousNo ratings yet
- Mother N ChildDocument5 pagesMother N ChildashariaserverNo ratings yet
- MCN II Trans TemplateDocument3 pagesMCN II Trans Templatecristinaparas04No ratings yet
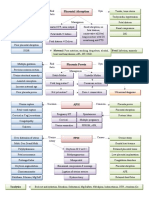
- Placental Abruption Schematic DiagramDocument2 pagesPlacental Abruption Schematic DiagramD CNo ratings yet
- Cerebral Palsy: Kernicterus (Infiltration of Bilirubin IntoDocument3 pagesCerebral Palsy: Kernicterus (Infiltration of Bilirubin IntoJulia SalvioNo ratings yet
- NCMB 219 ObDocument71 pagesNCMB 219 ObANGELICA MACASONo ratings yet
- Peran Wanita Dalam Pencegahan Stunting 22 April RevDocument23 pagesPeran Wanita Dalam Pencegahan Stunting 22 April Revtriana uji pamungkasNo ratings yet
- Postmaturity (Postterm) : High Risk NewbornDocument5 pagesPostmaturity (Postterm) : High Risk NewbornErika Marie CalucabNo ratings yet
- Antenatal Care Reviewer BSN 2BDocument4 pagesAntenatal Care Reviewer BSN 2BIrish EspinosaNo ratings yet
- Pregnancy at Risk NCM 109Document3 pagesPregnancy at Risk NCM 109kaycelyn jimenez100% (1)
- OBII - 15 Preterm Labor and BirthDocument8 pagesOBII - 15 Preterm Labor and BirthFelina CabadingNo ratings yet
- Complications of Pregnancy: Jose, Leana Louisse D. BSN 2BDocument14 pagesComplications of Pregnancy: Jose, Leana Louisse D. BSN 2BLiana Louisse JoseNo ratings yet
- NCM 109 NotesDocument45 pagesNCM 109 NotesJennie CortezNo ratings yet
- Olfubatch2017: "To Toil and Not To Seek For Rest... "Document4 pagesOlfubatch2017: "To Toil and Not To Seek For Rest... "Miguel C. DolotNo ratings yet
- Physical Diet/Lifestyl E Chemical Immunologic Environmenta L Hereditary Hormonal BiologicDocument1 pagePhysical Diet/Lifestyl E Chemical Immunologic Environmenta L Hereditary Hormonal BiologicJustine May GervacioNo ratings yet
- Teen Pregnancy ReferatDocument13 pagesTeen Pregnancy ReferatcokdebagusNo ratings yet
- L5 - Bleeding in Early Pregnancy (Miscarriage, Ectopic, Molar Pregnancy)Document3 pagesL5 - Bleeding in Early Pregnancy (Miscarriage, Ectopic, Molar Pregnancy)BrandonRyanF.MosidinNo ratings yet
- Pathophysiology of Preterm LaborDocument1 pagePathophysiology of Preterm LaborTine GuibaoNo ratings yet
- Maternal Note 1Document34 pagesMaternal Note 1JAN REY LANADONo ratings yet
- #1-NCM 109 - TransesDocument10 pages#1-NCM 109 - TransesJaimie BanaagNo ratings yet
- EDCs Infographics 22.2.20192 Low Doses MatterDocument1 pageEDCs Infographics 22.2.20192 Low Doses MatterAnnisa KoesnanNo ratings yet
- Cdp-Social 1CDocument18 pagesCdp-Social 1CJack RagodonNo ratings yet
- NCM 109 High Risk PregnancyDocument8 pagesNCM 109 High Risk PregnancyAngel MoncadaNo ratings yet
- Drug StudyDocument4 pagesDrug StudyYVETTE CLAIRE BORRESNo ratings yet
- Complications in Pregnancy & Labour 3: Pre-EclampsiaDocument1 pageComplications in Pregnancy & Labour 3: Pre-EclampsiajockorrNo ratings yet
- 109 Handout MaternalDocument22 pages109 Handout MaternalZyke NovenoNo ratings yet
- Welcome: Ms. Shesly P. Jose Ii Yr MSC NursingDocument94 pagesWelcome: Ms. Shesly P. Jose Ii Yr MSC NursingShesly PhilominaNo ratings yet
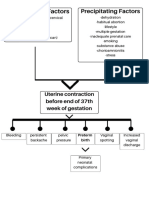
- Prefdisposing Factor Precipitating Factor: Fetal Distress/ DeathDocument2 pagesPrefdisposing Factor Precipitating Factor: Fetal Distress/ DeathRachelle AynNo ratings yet
- InfertilityDocument10 pagesInfertilityMuhammadR1No ratings yet
- NCM 109 Midterms - Infertility L2Document7 pagesNCM 109 Midterms - Infertility L2Leigh Angelika Dela CruzNo ratings yet
- Induction AND Augmentation OF LabourDocument42 pagesInduction AND Augmentation OF LabourDakshayini MbNo ratings yet
- Preterm LaborDocument1 pagePreterm LaborGabbi KimNo ratings yet
- Ectopic Pregnancy: Diagnosis Pathophysio Etiology Signs Management/ConsiderDocument4 pagesEctopic Pregnancy: Diagnosis Pathophysio Etiology Signs Management/ConsiderTin AteliagaNo ratings yet
- Psychology 110 Introduction To Psychology: Development - .Document6 pagesPsychology 110 Introduction To Psychology: Development - .surajoadNo ratings yet
- NCM 109 Module 1Document5 pagesNCM 109 Module 1Mery Ong BenitezNo ratings yet
- Assessment of High Risk PregnancyDocument8 pagesAssessment of High Risk PregnancyJessica Carmela Casuga100% (1)
- Case Study: "Patient Statement of Reason For Admission"Document8 pagesCase Study: "Patient Statement of Reason For Admission"mohamed mohamedNo ratings yet
- Preparation For Child BirthDocument41 pagesPreparation For Child BirthAngelica ErguizaNo ratings yet
- BNS RECORDS (Potrait)Document16 pagesBNS RECORDS (Potrait)CHRISTPHER LOURENCE C. MEMES0% (1)
- Bernabe Ncm109 LabDocument4 pagesBernabe Ncm109 LabKarl LintanNo ratings yet
- Covid 19 PregnancyDocument4 pagesCovid 19 PregnancyJasmine PerezNo ratings yet
- Shekhawati Form - FDocument2 pagesShekhawati Form - FArchit ChampanekarNo ratings yet
- Health Talk 1 Family PlanningDocument9 pagesHealth Talk 1 Family PlanningDeepika PatidarNo ratings yet
- Progestins AND AntiprogestinsDocument41 pagesProgestins AND AntiprogestinsdrfatimarizNo ratings yet
- Angle of Progression Measurements of Fetal Head at Term, A Systematic Comparison Between Open Magnetic Resonance Imaging and Transperineal UltrasoundDocument5 pagesAngle of Progression Measurements of Fetal Head at Term, A Systematic Comparison Between Open Magnetic Resonance Imaging and Transperineal UltrasoundNella SolanoNo ratings yet
- Contoh Artikel Buk RenoDocument5 pagesContoh Artikel Buk RenoDewita Wulan PratiwiNo ratings yet
- Birth Control PillsDocument1 pageBirth Control PillsBryan CaesarNo ratings yet
- Aisyah GDM ArticleDocument18 pagesAisyah GDM ArticleBesari Md DaudNo ratings yet
- Concept Paper - TP MidtermDocument6 pagesConcept Paper - TP MidtermMayAnnVillanuevaGallardoNo ratings yet
- Module 3 - Care of The Mother During The Intrapartal PeriodDocument14 pagesModule 3 - Care of The Mother During The Intrapartal PeriodKatie HolmesNo ratings yet
- Post-Partum (New)Document111 pagesPost-Partum (New)coosa liquorsNo ratings yet
- ErasinfographicDocument1 pageErasinfographicapi-641786123No ratings yet
- MCQs 1Document6 pagesMCQs 1Ali Nawaz AyubiNo ratings yet
- Customs and Taboos of Bidayuh CommunityDocument13 pagesCustoms and Taboos of Bidayuh CommunityMarlon Abdullah100% (1)
- Paternity, Surrogacy and Protection of ChildDocument23 pagesPaternity, Surrogacy and Protection of ChildBidhan PoudyalNo ratings yet
- NCP RomeroDocument3 pagesNCP RomeroJear RomeroNo ratings yet
- B5124Document91 pagesB5124Gede JayaNo ratings yet
- Risk For InjuryDocument3 pagesRisk For InjuryAvery SandsNo ratings yet
- San Pablo (DILG) - GAD Plan 2021Document12 pagesSan Pablo (DILG) - GAD Plan 2021CA T HeNo ratings yet
- Program EmasDocument8 pagesProgram EmasSavitri FazriNo ratings yet
- Twin TDocument30 pagesTwin TmaezuNo ratings yet
- Preterm Labor Case Analysis For High Risk AntepartumDocument2 pagesPreterm Labor Case Analysis For High Risk AntepartumJOPAR JOSE C. RAMOSNo ratings yet
- Adolescent Reproductive Health (ARH) Teenage Pregnancy Prevention AwarenessDocument3 pagesAdolescent Reproductive Health (ARH) Teenage Pregnancy Prevention AwarenessJasmin GallaNo ratings yet
- Mapa Ingles RPMDocument1 pageMapa Ingles RPMDaniela RodriguezNo ratings yet
- Selective Versus Routine Use of Episiotomy For Vaginal Birth (Review)Document77 pagesSelective Versus Routine Use of Episiotomy For Vaginal Birth (Review)Bella DirkNo ratings yet
- s40748 019 0103 yDocument7 pagess40748 019 0103 yputri vinia /ilove cuteNo ratings yet
- How To Manage Early Embryonic Death: Tom A.E. Stout, Vetmb, PHDDocument3 pagesHow To Manage Early Embryonic Death: Tom A.E. Stout, Vetmb, PHDMittu KurianNo ratings yet