You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Best of Five Mcqs For The Gastroenterology Sce PDFDocument315 pagesBest of Five Mcqs For The Gastroenterology Sce PDFSabry Anees100% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Colon Cleansing Kit Users GuideDocument74 pagesColon Cleansing Kit Users GuideYoungBody0% (1)
- Diabetic Diet Ebook Toma'sDocument178 pagesDiabetic Diet Ebook Toma'sHetal Patel100% (1)
- Notes From USMLE Step 1 Goljan LecturesDocument40 pagesNotes From USMLE Step 1 Goljan Lecturesgb100% (1)
- ICPC-2 - EnglishDocument2 pagesICPC-2 - EnglishEddieNo ratings yet
- Information On Diabetes Explicit Misery Are Expected To Work On The Nature of Diabetes CareDocument2 pagesInformation On Diabetes Explicit Misery Are Expected To Work On The Nature of Diabetes CareBashar Al-AhmadNo ratings yet
- Nursing Seminar 1 SAS Session 22Document9 pagesNursing Seminar 1 SAS Session 22ZiaNo ratings yet
- BMJ g7620 FullDocument10 pagesBMJ g7620 FullRui PenedaNo ratings yet
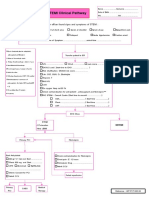
- STEMI Clinical PathwayDocument1 pageSTEMI Clinical PathwayKanoknun PisitpatcaragulNo ratings yet
- MYIASISDocument2 pagesMYIASISMirna HusseinNo ratings yet
- Upper Limb OrthosisDocument47 pagesUpper Limb OrthosisPraneethaNo ratings yet
- Presentation 1Document23 pagesPresentation 1Anonymous HK3LyOqR2g100% (1)
- Padlet Lesson PlanDocument4 pagesPadlet Lesson Planapi-273579197No ratings yet
- Cystic Fibrosis: SymptomsDocument2 pagesCystic Fibrosis: SymptomsMehrul Singh RanavatNo ratings yet
- Management of Disease Through Yoga and Nature CureDocument17 pagesManagement of Disease Through Yoga and Nature CureAnushree ChauhanNo ratings yet
- Spleen and Liver Sur LecDocument14 pagesSpleen and Liver Sur LecYA M AYNo ratings yet
- SiddaDocument28 pagesSiddaBala Kiran GaddamNo ratings yet
- Pediatric TuberculosisDocument19 pagesPediatric TuberculosisRajath Kumar K R KNo ratings yet
- Toxic Shock Syndrome UHL Childrens GuidelineDocument12 pagesToxic Shock Syndrome UHL Childrens GuidelineBariša KiršnerNo ratings yet
- Neuromyelitis Optica Spectrum Disorders10Document40 pagesNeuromyelitis Optica Spectrum Disorders10Barbara LomeNo ratings yet
- Staphylococcus & StreptococcusDocument100 pagesStaphylococcus & StreptococcusFahim NadvyNo ratings yet
- Presentation On Behavioral DisorderDocument81 pagesPresentation On Behavioral DisorderTanviNo ratings yet
- 40 - Laginlin v. WCC G.R. No. L-45785Document5 pages40 - Laginlin v. WCC G.R. No. L-45785Shash BernardezNo ratings yet
- Clinically Isolated Syndrome and Early Relapsing Multiple SclerosisDocument19 pagesClinically Isolated Syndrome and Early Relapsing Multiple Sclerosisnight.shadowNo ratings yet
- Complications of PrematurityDocument11 pagesComplications of PrematurityMarvin Machuca RamosNo ratings yet
- Aortic RegurgitationDocument18 pagesAortic RegurgitationAbdur RaqibNo ratings yet
- 49271Document29 pages49271Raghav RathiNo ratings yet
- MY THOUGHTS ABOUT "A Beautiful Mind": Daro, Farhannah T. Bsn-3Document1 pageMY THOUGHTS ABOUT "A Beautiful Mind": Daro, Farhannah T. Bsn-3AnnahNo ratings yet
- Immunology and Serology TestsDocument2 pagesImmunology and Serology TestsPearlregine Cianne MirandaNo ratings yet