You might also like
- Protein Metabolism and Acids SamyA1Document170 pagesProtein Metabolism and Acids SamyA1Abby RahmanNo ratings yet
- Amino Acid Catabolism Between OrgansDocument44 pagesAmino Acid Catabolism Between OrgansFarhati MardhiyahNo ratings yet
- Amino Acid MetabolismDocument30 pagesAmino Acid MetabolismMeddebateNo ratings yet
- Fatty Acid Synthesis 11.12.19Document18 pagesFatty Acid Synthesis 11.12.19Sanreet Randhawa100% (1)
- Hexose Monophosphate Shunt CHEM3119"TITLE"Biometabolism Lecture on HMP Shunt and G6PD DeficiencyDocument18 pagesHexose Monophosphate Shunt CHEM3119"TITLE"Biometabolism Lecture on HMP Shunt and G6PD DeficiencyAbdul Jabbar Abdul JabbarNo ratings yet
- Biosynthesis of of NucleotidesDocument48 pagesBiosynthesis of of NucleotidesBabul Aktar100% (1)
- Understanding Metabolism of CarbohydratesDocument48 pagesUnderstanding Metabolism of CarbohydratesAbdullah TheNo ratings yet
- Metabolism of Purine & Pyrimidine NucleotidesDocument38 pagesMetabolism of Purine & Pyrimidine NucleotidesShimmering MoonNo ratings yet
- Integration of Metabolism PathwaysDocument68 pagesIntegration of Metabolism PathwaysCahyani Tiara Safitri100% (1)
- Biochemistry of Kidneys and UrineDocument18 pagesBiochemistry of Kidneys and UrineAndrias PutriNo ratings yet
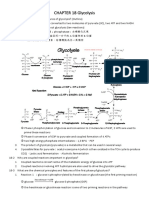
- CHAPTER 18 GlycolysisDocument10 pagesCHAPTER 18 Glycolysis楊畯凱No ratings yet
- Biochemistry of Digestive SystemDocument55 pagesBiochemistry of Digestive SystemSyam UnhasNo ratings yet
- Amino AcidsDocument32 pagesAmino AcidsStephen Leonel100% (1)
- Nucleotide Biosynthesis: Functions, Pathways and RegulationDocument23 pagesNucleotide Biosynthesis: Functions, Pathways and RegulationSaad KazmiNo ratings yet
- Some Biochem MnemonicsDocument8 pagesSome Biochem MnemonicsMikey PalominoNo ratings yet
- Nucleic Acid MetabolismDocument23 pagesNucleic Acid MetabolismMSc Biotech/MicroNo ratings yet
- Glycolysis NotesDocument2 pagesGlycolysis NotesAnsley Ellen BarfieldNo ratings yet
- Nucleotide Metabolism SummaryDocument10 pagesNucleotide Metabolism SummaryRonak UpadhyayNo ratings yet
- ProteinDocument39 pagesProteinNICHOLE MOJELLO100% (2)
- Classification of Protein Based On CompositionDocument4 pagesClassification of Protein Based On CompositionHambaliNo ratings yet
- Biology OxidationDocument50 pagesBiology Oxidationderhangker100% (3)
- Biological Oxidation Reactions and EnzymesDocument11 pagesBiological Oxidation Reactions and EnzymesJo AnnNo ratings yet
- Urea CycleDocument11 pagesUrea CycleRohit VinayNo ratings yet
- Protein MetabolismDocument6 pagesProtein MetabolismGeline Dela RosaNo ratings yet
- Heme Metabolism PDFDocument19 pagesHeme Metabolism PDFAnonymous jW7BU44ACNo ratings yet
- Ni Nyoman Ayu Dewi Dept. of Biochemistry, Faculty of Medicine Udayana University Ayu - Dewi@unud - Ac.idDocument37 pagesNi Nyoman Ayu Dewi Dept. of Biochemistry, Faculty of Medicine Udayana University Ayu - Dewi@unud - Ac.idWida Utami100% (1)
- Chapter 2 - Metabolism & Bioenergetics (Part 2) PDFDocument69 pagesChapter 2 - Metabolism & Bioenergetics (Part 2) PDFdarren100% (2)
- Regulation of Gluconeogenesis and Glycogen MetabolismDocument35 pagesRegulation of Gluconeogenesis and Glycogen MetabolismdanielachynaNo ratings yet
- Purine & Pyrimidine MetabolismDocument22 pagesPurine & Pyrimidine MetabolismManda100% (1)
- CARBOHYDRATESDocument38 pagesCARBOHYDRATESgulrukh100% (3)
- Lec Notes Carbohydrate Metabolism Glycolysis Kreb Cycle ETCDocument12 pagesLec Notes Carbohydrate Metabolism Glycolysis Kreb Cycle ETCJonah Micah MangacoNo ratings yet
- 41 & 42 - Nucleic Acid MetabolismDocument56 pages41 & 42 - Nucleic Acid MetabolismMădă Claws100% (1)
- NPN Compounds: Urea, Creatinine, Uric Acid & AmmoniaDocument37 pagesNPN Compounds: Urea, Creatinine, Uric Acid & AmmoniaMustafa KhandgawiNo ratings yet
- Atp Synthesis by Cellular Respiration AT P: Caroline SueperDocument9 pagesAtp Synthesis by Cellular Respiration AT P: Caroline SueperCaroline SueperNo ratings yet
- Chapter Three Amino Acids and Peptides: Paul D. Adams - University of ArkansasDocument27 pagesChapter Three Amino Acids and Peptides: Paul D. Adams - University of ArkansasSheila GarciaNo ratings yet
- Gluconeogenesis & HMP Shunt ExplainedDocument36 pagesGluconeogenesis & HMP Shunt ExplainedAshish K Joy100% (1)
- Disorders of Purine and Pyrimidine MetabolismDocument17 pagesDisorders of Purine and Pyrimidine Metabolismtanmay mehtaNo ratings yet
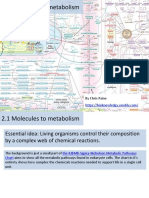
- 2.1 Molecules To Metabolism-STUDENTDocument54 pages2.1 Molecules To Metabolism-STUDENTAngel Alexandra SiregarNo ratings yet
- Haemoglobin: DR Nilesh Kate MBBS, MD Associate ProfDocument31 pagesHaemoglobin: DR Nilesh Kate MBBS, MD Associate ProfMarcellia100% (1)
- Citric Acid Cycle Enzyme Pyruvate DehydrogenaseDocument33 pagesCitric Acid Cycle Enzyme Pyruvate Dehydrogenasesultan khabeeb100% (1)
- S13.CHO .MetabolismDocument18 pagesS13.CHO .MetabolismGhea Jovita SinagaNo ratings yet
- Metabolic Pathway of Carbohydrate and GlycolysisDocument22 pagesMetabolic Pathway of Carbohydrate and GlycolysisDarshansinh MahidaNo ratings yet
- 10 Steps Glycolysis ExplainedDocument8 pages10 Steps Glycolysis Explaineddani2703No ratings yet
- 2 Bioenergetics and Oxidative Metabolism IDocument3 pages2 Bioenergetics and Oxidative Metabolism ILinus LiuNo ratings yet
- Protein PPT PrelimDocument8 pagesProtein PPT PrelimMacchi MagsNo ratings yet
- Understanding Steroidal HormonesDocument23 pagesUnderstanding Steroidal HormonesJazab ChohanNo ratings yet
- HMPDocument44 pagesHMPraanja2No ratings yet
- Cofactor and CoenzymeDocument24 pagesCofactor and CoenzymeBIDIN100% (1)
- Sphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeDocument12 pagesSphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeUzac BenuNo ratings yet
- 6.1 Types of NutritionDocument11 pages6.1 Types of NutritionNoor Hidayah SambliNo ratings yet
- Glycogen MetabolismDocument23 pagesGlycogen Metabolismessa100% (1)
- Metabolism of LipidsDocument47 pagesMetabolism of LipidsMarwahNo ratings yet
- Uronic Acid PathwayDocument4 pagesUronic Acid PathwayAlen Arthur100% (2)
- Cellular Respiration PathwaysDocument5 pagesCellular Respiration PathwaysStealthstr1keNo ratings yet
- Git Biochemistry of GitDocument9 pagesGit Biochemistry of GitSibatNo ratings yet
- Metabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaDocument60 pagesMetabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaAmanda PutriNo ratings yet
- Purine Metabolism de Novo Synthesis and Salvage Pathway, 2015Document28 pagesPurine Metabolism de Novo Synthesis and Salvage Pathway, 2015Tehreem NadeemNo ratings yet
- Hexose Mono Phosphate (HMP) ShuntDocument28 pagesHexose Mono Phosphate (HMP) ShuntVishesh JainNo ratings yet
- Lecture on amino acid metabolism and the urea cycleDocument41 pagesLecture on amino acid metabolism and the urea cycleQamar QamarNo ratings yet
- The General and Special Senses GuideDocument40 pagesThe General and Special Senses GuideSanjana VasistNo ratings yet
- 734 Visual Pathway LesionsDocument25 pages734 Visual Pathway LesionsNarendra N NaruNo ratings yet
- Biochemistry Metabolic Pathways OverviewDocument32 pagesBiochemistry Metabolic Pathways OverviewSanjana VasistNo ratings yet
- Viva in Anatomy, Physiology and Biochemistry (2010) (PDF)Document345 pagesViva in Anatomy, Physiology and Biochemistry (2010) (PDF)KAmil71% (31)
- DIPPR Compound List 2014 ChemicalsDocument122 pagesDIPPR Compound List 2014 ChemicalsWink ElliottNo ratings yet
- Drug Metabolism: Dr. Amal BelaidDocument28 pagesDrug Metabolism: Dr. Amal BelaidMustafa RihanNo ratings yet
- Nomenclature of Polyfunctional Organic CompoundsDocument6 pagesNomenclature of Polyfunctional Organic CompoundsJuan Carlos100% (2)
- Ethylene Production GuideDocument53 pagesEthylene Production Guidekingcobra008100% (5)
- Piccs 2012 PDFDocument1,614 pagesPiccs 2012 PDFAnnabelle GuilingNo ratings yet
- Table 1 Average Contents of Esters (N 3, Equivalent of 3-Octanol) and Their Distribution Ranges (In Parenthesis) in The Fruits of 39 Melon CultivarsDocument3 pagesTable 1 Average Contents of Esters (N 3, Equivalent of 3-Octanol) and Their Distribution Ranges (In Parenthesis) in The Fruits of 39 Melon CultivarsyassinharanNo ratings yet
- Advances in N- and O-Demethylation MethodsDocument26 pagesAdvances in N- and O-Demethylation MethodsAnonymous 4KaJRMNo ratings yet
- POLYMERIZATION PROCESSESDocument38 pagesPOLYMERIZATION PROCESSESutami10No ratings yet
- Aldehydes and Ketones ReactionsDocument9 pagesAldehydes and Ketones ReactionsKudzayi Tusaumwe100% (1)
- Total Synthesis of CorylidinDocument7 pagesTotal Synthesis of CorylidinHafiz Usama ImamNo ratings yet
- Aplikasi OrganologamDocument8 pagesAplikasi OrganologamSUCI WIDIANINGSIHNo ratings yet
- Kimia Lipida 2017 Setya - D3Document44 pagesKimia Lipida 2017 Setya - D3Anggito PrayogaNo ratings yet
- Biomolecules and Polymers TheoryDocument32 pagesBiomolecules and Polymers Theoryamanky341No ratings yet
- Chapter 2 - Bronsted-Lowry TheoryDocument19 pagesChapter 2 - Bronsted-Lowry TheoryAcidri AbdulkarimNo ratings yet
- SL Paper 1: CH CH +H CH + BR CH +HBR CH + BR CH BR + H CH +BR CH BRDocument8 pagesSL Paper 1: CH CH +H CH + BR CH +HBR CH + BR CH BR + H CH +BR CH BRPisosNo ratings yet
- Surfactants: An IMS (ISO 9001:2015 ISO 14001: 2015 and OHSAS 18001:2007) Certified CompanyDocument12 pagesSurfactants: An IMS (ISO 9001:2015 ISO 14001: 2015 and OHSAS 18001:2007) Certified CompanyChetas BiochemNo ratings yet
- Alkanes, Alkenes, AlkynesDocument7 pagesAlkanes, Alkenes, AlkynesMuhammad Hasnain AliNo ratings yet
- thiols, ethers, and sulfidesDocument56 pagesthiols, ethers, and sulfidesgsy2023-9150-52879No ratings yet
- Attempt All The Questions (2) All Questions Carry Marks As IndicatedDocument1 pageAttempt All The Questions (2) All Questions Carry Marks As IndicatedDAMBALENo ratings yet
- CHEM 109A: Organic ChemistryDocument26 pagesCHEM 109A: Organic ChemistryStarcraft2shit 2sNo ratings yet
- AMIDESDocument9 pagesAMIDESJhonnie Mae OtacanNo ratings yet
- MIchael Addition Using K2CO3 As A CatalystDocument3 pagesMIchael Addition Using K2CO3 As A Catalystredevol7No ratings yet
- Alkyl Halide NotesDocument112 pagesAlkyl Halide NotesRaval sagarNo ratings yet
- Chemistry 12 Homework Assignment 3-1Document7 pagesChemistry 12 Homework Assignment 3-1erstz00g100% (1)
- Efficient Method For The Direct Preparation of Amides From Carboxylic Acids Using Tosyl Chloride Under Solvent-Free ConditionsDocument4 pagesEfficient Method For The Direct Preparation of Amides From Carboxylic Acids Using Tosyl Chloride Under Solvent-Free ConditionsAhmed ElkamhawyNo ratings yet
- Organometallic Compounds (OMCsDocument34 pagesOrganometallic Compounds (OMCsMelissa ChehwaneNo ratings yet
- Prathyusha RSCDocument8 pagesPrathyusha RSCDr-Prathyusha VadlamudiNo ratings yet
- Quaternary Ammonium CompoundsDocument5 pagesQuaternary Ammonium CompoundsRana SabNo ratings yet
- SUMMATIVE BSED3 RiliDocument6 pagesSUMMATIVE BSED3 RiliJohn Bernard RiliNo ratings yet
- Goc 02 SheetDocument62 pagesGoc 02 SheetmikcNo ratings yet