You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nursing Pharmacology Sample Exam QuestionsDocument3 pagesNursing Pharmacology Sample Exam QuestionsDhreambhig Ahrchorphul100% (1)
- Cleft Lip and PalateDocument8 pagesCleft Lip and PalateSHEILA MAE SACLOTNo ratings yet
- KDIGO Transplantation GuidelinesDocument2 pagesKDIGO Transplantation GuidelinesSoteres VrachnesNo ratings yet
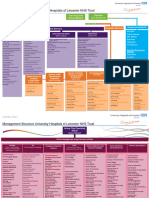
- 358-5215538-CSI-A - University Hospitals of Leicester Management StructureDocument4 pages358-5215538-CSI-A - University Hospitals of Leicester Management Structureantonymeghna36No ratings yet
- Epo66 A: 95@lto 6oidaDocument2 pagesEpo66 A: 95@lto 6oidaTharaka GamageNo ratings yet
- Post Test On Needle Stick InjuryDocument4 pagesPost Test On Needle Stick InjurysunitapuniaNo ratings yet
- Advanced Ultrasound-Guided Interventions For TenopathyDocument16 pagesAdvanced Ultrasound-Guided Interventions For TenopathyJuanMa Correa SanabriaNo ratings yet
- Combination of DrugDocument4 pagesCombination of Drugabirami sNo ratings yet
- Social Studies SBADocument12 pagesSocial Studies SBASamuraiメ.No ratings yet
- Dry ARMD Oral SupplementsDocument5 pagesDry ARMD Oral SupplementsVishNo ratings yet
- Husi:: Notifikasaun Moras Ka Moras Ne'ebe Akontese Ho SurtuDocument18 pagesHusi:: Notifikasaun Moras Ka Moras Ne'ebe Akontese Ho SurtuTīťťhūś Cårvåłhø100% (1)
- K-Flam (Diclofenac Potassium) SachetsDocument92 pagesK-Flam (Diclofenac Potassium) SachetsAmolNo ratings yet
- Cryotherapy 130116134934 Phpapp01 PDFDocument57 pagesCryotherapy 130116134934 Phpapp01 PDFMichael SelvarajNo ratings yet
- Laparoscopy: Shenillee Burgess Reyad HoseinDocument31 pagesLaparoscopy: Shenillee Burgess Reyad HoseinShenillee BurgessNo ratings yet
- ChainingDocument38 pagesChainingKhadija ArshadNo ratings yet
- Rehabilitation of Adults With Upper-Limb AmputationsDocument59 pagesRehabilitation of Adults With Upper-Limb AmputationsSameeha AbbassNo ratings yet
- Health - UROD (About Heroin Detoxification)Document79 pagesHealth - UROD (About Heroin Detoxification)GuacoponNo ratings yet
- GinecologíaDocument5 pagesGinecologíaLeonela SánchezNo ratings yet
- The Child With Neuromuscular or Muscular Dysfunction NOTESDocument27 pagesThe Child With Neuromuscular or Muscular Dysfunction NOTESERIKA BOOTS CABALUNANo ratings yet
- PUC-WOE Done But Not Imported - ABMC019Document40 pagesPUC-WOE Done But Not Imported - ABMC019ManishNo ratings yet
- IntroClin - Pedia IE, CVGHDocument11 pagesIntroClin - Pedia IE, CVGHAnnbe BarteNo ratings yet
- Superbugs in Our HospitalsDocument2 pagesSuperbugs in Our Hospitalstummalapalli venkateswara raoNo ratings yet
- Fluid & Elecrolytes Management in NewbornsDocument42 pagesFluid & Elecrolytes Management in NewbornsDR.MAULIK SHAHNo ratings yet
- Amlodipine Drug StudyDocument2 pagesAmlodipine Drug StudyJoseph Dann Enero Jr.100% (3)
- Perform Basic First Aid ProceduresDocument76 pagesPerform Basic First Aid ProceduresGlenn ClementeNo ratings yet
- Drug StudyDocument5 pagesDrug StudyRai D. MacapantonNo ratings yet
- NCS EMG Patient Information GuideDocument1 pageNCS EMG Patient Information GuideCarolina PNo ratings yet
- Konsep KecemasanDocument12 pagesKonsep Kecemasangajah purbaNo ratings yet
- Bol Anali̇zli̇ C.FDocument16 pagesBol Anali̇zli̇ C.FTalipNo ratings yet
- CBT For Anxiety Disorders and DepressionDocument5 pagesCBT For Anxiety Disorders and DepressionCristina ColoteloNo ratings yet