You might also like
- Methylergonovine Med TemplateDocument1 pageMethylergonovine Med Templateel shilohNo ratings yet
- 120 HAAD Exam QuestionsDocument10 pages120 HAAD Exam QuestionsConsolacion Binarao Dolores50% (8)
- Luteal Phase Defect: Dr. Priyankur Roy Consultant Infertility Specialist & Laparoscopic SurgeonDocument45 pagesLuteal Phase Defect: Dr. Priyankur Roy Consultant Infertility Specialist & Laparoscopic SurgeonPriyankur RoyNo ratings yet
- Lyn Watson Level TwoDocument4 pagesLyn Watson Level TwoAlastair HarrisNo ratings yet
- Management of Pelvic Girdle Pain in Pregnancy and Post-PartumDocument27 pagesManagement of Pelvic Girdle Pain in Pregnancy and Post-PartumrahmawatusNo ratings yet
- Manual Techniques For The Knee - Katie CusackDocument10 pagesManual Techniques For The Knee - Katie CusacknataleebellaNo ratings yet
- Infeksi Saluran KemihDocument35 pagesInfeksi Saluran KemihLestari Amelia AdmNo ratings yet
- Case Study (Aub)Document16 pagesCase Study (Aub)Lucila Lugo0% (2)
- Pelvic Dysfunction in Men: Diagnosis and Treatment of Male Incontinence and Erectile DysfunctionFrom EverandPelvic Dysfunction in Men: Diagnosis and Treatment of Male Incontinence and Erectile DysfunctionNo ratings yet
- The Role of Hormone in ParturitionDocument36 pagesThe Role of Hormone in ParturitionDiana HayatiNo ratings yet
- Acute Diffuse Otitis ExternaDocument36 pagesAcute Diffuse Otitis ExternaIlham Isnin Dolyanov HasibuanNo ratings yet
- Teknik Anamnesis & Pemeriksaan Fisik Umum (Dr. Rini Bachtiar, SP - PD)Document79 pagesTeknik Anamnesis & Pemeriksaan Fisik Umum (Dr. Rini Bachtiar, SP - PD)nurfatrianiNo ratings yet
- Range of Motion Technique: by Anisa Altaf 18205 Presented To DR Sumeet Kumar Therapeutic ExcerciseDocument22 pagesRange of Motion Technique: by Anisa Altaf 18205 Presented To DR Sumeet Kumar Therapeutic ExcerciseArsal MushtaqNo ratings yet
- Vovulusoriginal Copy 121028055752 Phpapp01Document37 pagesVovulusoriginal Copy 121028055752 Phpapp01Bheru LalNo ratings yet
- Gannguan PubertasDocument56 pagesGannguan PubertasAde Yosdi PutraNo ratings yet
- Chronic Pelvic Pain2010Document48 pagesChronic Pelvic Pain2010Feruza SultanmuratovaNo ratings yet
- Kegel Handout PDFDocument1 pageKegel Handout PDFMini ManojNo ratings yet
- Diastasis RectiDocument14 pagesDiastasis RectiVitra Mayaa100% (2)
- DVT & Varicose VeinsDocument30 pagesDVT & Varicose VeinsMargaret Xaira Rubio MercadoNo ratings yet
- Pregnancy Made Confortable With Yoga & Dietetics: Yogic exercises & nutrition to make motherhood easyFrom EverandPregnancy Made Confortable With Yoga & Dietetics: Yogic exercises & nutrition to make motherhood easyNo ratings yet
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 pagesNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenNo ratings yet
- Amnioinfusion - LEODocument16 pagesAmnioinfusion - LEOtapayanaNo ratings yet
- ConstipationDocument22 pagesConstipationash ash100% (1)
- Hydrosalpinx MBDocument30 pagesHydrosalpinx MBverhaniNo ratings yet
- Anatomi Panggul Dan UkurannyaDocument40 pagesAnatomi Panggul Dan UkurannyaGiritama IrwantoroNo ratings yet
- Neo BladderDocument32 pagesNeo Bladderbelieveme030589No ratings yet
- Cervicogenic Headache PDFDocument13 pagesCervicogenic Headache PDFSuganya Balachandran100% (2)
- AnatDocument119 pagesAnatGanesh RasalNo ratings yet
- Sacrum Self Study GuideDocument24 pagesSacrum Self Study GuideMichel BakkerNo ratings yet
- Levator Ani SyndromeDocument24 pagesLevator Ani SyndromeKavya KavyasujathaNo ratings yet
- Female Pelvic RelaxationDocument28 pagesFemale Pelvic RelaxationHafid IqbalNo ratings yet
- Physiology of Micturition by DR - JawariaDocument20 pagesPhysiology of Micturition by DR - JawariaHifza Faqeer KambohNo ratings yet
- Urinary IncontinenceDocument66 pagesUrinary Incontinencedr_asaleh100% (1)
- Suprapubic Catheter Bladder TrainingDocument17 pagesSuprapubic Catheter Bladder TrainingOrmias PratamaNo ratings yet
- Non-Surgical and Surgical Management of Pelvic OrgDocument10 pagesNon-Surgical and Surgical Management of Pelvic OrgAhmed AnwarNo ratings yet
- Women With Cronic Pelvic Pain. An Osteopathic Approach PDFDocument3 pagesWomen With Cronic Pelvic Pain. An Osteopathic Approach PDFHapplo82No ratings yet
- Uro DynamicsDocument64 pagesUro DynamicsSri HariNo ratings yet
- Cystostomy NewDocument32 pagesCystostomy Newkuncupcupu1368No ratings yet
- Tugas SC Vs Histerotomi Vs Laparotomi Ambil Anak Aji PatriajatiDocument3 pagesTugas SC Vs Histerotomi Vs Laparotomi Ambil Anak Aji PatriajatiAji PatriajatiNo ratings yet
- Bladder Substitution and Urinary DiversionDocument58 pagesBladder Substitution and Urinary DiversionlifespotNo ratings yet
- Retractile Testis PDFDocument6 pagesRetractile Testis PDFDella Elvina RoeslandNo ratings yet
- International Journal of Ayurveda and Pharma ResearchDocument5 pagesInternational Journal of Ayurveda and Pharma Researchtanmai nooluNo ratings yet
- 04pelvic Floor Physiotherapy For The Management of Incontinence by Kealy France (1 Jun 2016)Document44 pages04pelvic Floor Physiotherapy For The Management of Incontinence by Kealy France (1 Jun 2016)RajiNo ratings yet
- Hallmark of Cancer: Nur MahmudahDocument40 pagesHallmark of Cancer: Nur MahmudahFahmi SuhandinataNo ratings yet
- Cystoscopy: A Guide For WomenDocument2 pagesCystoscopy: A Guide For Womenmonir61No ratings yet
- IV - Modul 12B - Nutrisi ParenteralDocument44 pagesIV - Modul 12B - Nutrisi Parenteralellyn fajriahNo ratings yet
- Perdarahan Pasca SalinDocument36 pagesPerdarahan Pasca SalinbennyrolandnababanNo ratings yet
- Shoulder Impingement SyndromeDocument37 pagesShoulder Impingement SyndromeDADDYGUS100% (1)
- Passive Scapular Adduction TestDocument15 pagesPassive Scapular Adduction Testapi-468597987No ratings yet
- Intravenous Urography. RADIOPEDIADocument2 pagesIntravenous Urography. RADIOPEDIAdokter muda100% (1)
- Mnemonic Vacum Dan Forcep NewDocument2 pagesMnemonic Vacum Dan Forcep NewsinggehNo ratings yet
- Omphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Document17 pagesOmphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Rully Riyan DikaNo ratings yet
- Diastasis Rectus Abdominis: Patient InformationDocument8 pagesDiastasis Rectus Abdominis: Patient InformationJames McInerneyNo ratings yet
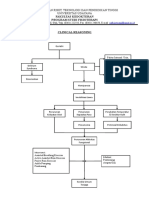
- Clinical ReasoningDocument1 pageClinical ReasoningIda Bagus Gde Dharma DhyaksaNo ratings yet
- Diagnosis and Management of Pelvic Organ ProlapseDocument47 pagesDiagnosis and Management of Pelvic Organ ProlapseWindy Puspa Kusumah100% (1)
- Uroflowmetry InterpretationDocument4 pagesUroflowmetry InterpretationMeryl PulcheriaNo ratings yet
- Assessment of Fetal Well BeingDocument46 pagesAssessment of Fetal Well BeingAumrin Fathima100% (1)
- Bleeding in Early Pregnancy Slide WorldDocument57 pagesBleeding in Early Pregnancy Slide Worlddashing_ritamNo ratings yet
- Urethral Stricture DiseaseDocument9 pagesUrethral Stricture DiseaseIntanAgustiFernandesNo ratings yet
- Physiology of Labor: Ribkhi Amalia Putri Ganot SumulyoDocument48 pagesPhysiology of Labor: Ribkhi Amalia Putri Ganot SumulyoImelda AtikaNo ratings yet
- Pelvic Floor Anatomy and The Surgery of Pulsion EnterocoeleDocument185 pagesPelvic Floor Anatomy and The Surgery of Pulsion EnterocoeleSamir CastilloNo ratings yet
- Narrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowDocument12 pagesNarrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowLéa Cinthia Silva do NascimentoNo ratings yet
- Stenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandStenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Anaplasma Marginale: Infection in A Buffalo: A Case ReportDocument3 pagesAnaplasma Marginale: Infection in A Buffalo: A Case ReportshivarajuNo ratings yet
- Hema II Chapter 3 - Anemiarev - ATDocument154 pagesHema II Chapter 3 - Anemiarev - AThannigadah7No ratings yet
- GEMP 3 2020 Advice & TestsDocument52 pagesGEMP 3 2020 Advice & TestsTresor KabambaNo ratings yet
- Clinical Accessories Portfolio R860Document8 pagesClinical Accessories Portfolio R860TATA ARROYAVENo ratings yet
- DR Bhavini Sandip Shah Director: Microbiology Department of Microbiology Neuberg Supratech Labs AhmedabadDocument49 pagesDR Bhavini Sandip Shah Director: Microbiology Department of Microbiology Neuberg Supratech Labs Ahmedabadkrutarth shahNo ratings yet
- Diseases of ImmunityDocument13 pagesDiseases of ImmunityRose AnnNo ratings yet
- 3 - Lung Meridian PointsDocument3 pages3 - Lung Meridian PointsClaudiaAlexandruNo ratings yet
- Hospital La Comunidad de Santa Rosa: Chapter I: Problem and Its SettingsDocument15 pagesHospital La Comunidad de Santa Rosa: Chapter I: Problem and Its SettingsMeynard MagsinoNo ratings yet
- Opioid Free Anesthesia A Different Regard To.98965 PDFDocument6 pagesOpioid Free Anesthesia A Different Regard To.98965 PDFgabriel herreraNo ratings yet
- Epidemiological Characterization of Dermatomycosis in EthiopiaDocument7 pagesEpidemiological Characterization of Dermatomycosis in EthiopiaMini LaksmiNo ratings yet
- MCQ FinalDocument10 pagesMCQ FinalFow 40% (1)
- Hema I Chapter 12 - ESRDocument30 pagesHema I Chapter 12 - ESRTesfaNo ratings yet
- Presentation TrypanosomiasisDocument16 pagesPresentation Trypanosomiasischiara.ruinaNo ratings yet
- EpisiotomyDocument18 pagesEpisiotomyAnnapurna DangetiNo ratings yet
- ICDAS Dental CariesDocument6 pagesICDAS Dental CariestulusNo ratings yet
- FIRST AID Is The Immediate Care Given To A Person Who Have Been Injured or Suddenly Taken IllDocument4 pagesFIRST AID Is The Immediate Care Given To A Person Who Have Been Injured or Suddenly Taken IllNat CatalanNo ratings yet
- Neuromuscular Blocking AgentsnewDocument22 pagesNeuromuscular Blocking Agentsnewvinay0717100% (1)
- Updated Unang Yakap Checklist 1Document3 pagesUpdated Unang Yakap Checklist 1Myrel Cedron TucioNo ratings yet
- Vero CellDocument2 pagesVero CellYawar AbbasNo ratings yet
- Zhongfeng Liv-4: Middle SealDocument2 pagesZhongfeng Liv-4: Middle Sealray72roNo ratings yet
- Simulation Based Training For Anaesthesia ResidentsDocument8 pagesSimulation Based Training For Anaesthesia ResidentsSajal SahaNo ratings yet
- Health Consideration at Work Place: Airborne DiseasesDocument12 pagesHealth Consideration at Work Place: Airborne DiseasesvishwaNo ratings yet
- A 22 Yrs Old Female With Progressive MuscleDocument25 pagesA 22 Yrs Old Female With Progressive MuscleTamzid Rabby TanmoyNo ratings yet
- Abnormal Labor. BBBB WWPPTXDocument53 pagesAbnormal Labor. BBBB WWPPTXHamss Ahmed100% (2)
- Intro To Patient Care Exam 2 Content QuestionsDocument81 pagesIntro To Patient Care Exam 2 Content QuestionsAlyss Wallschleger50% (2)
- Research Proposal s2Document2 pagesResearch Proposal s2api-451543560No ratings yet
- Resume Anna BalancioDocument3 pagesResume Anna Balanciojihn isis tengcoNo ratings yet