You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Class 5 HeadachesDocument14 pagesClass 5 Headacheswitlinger88No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cristina Barsolo VS SSSDocument2 pagesCristina Barsolo VS SSSHasmer Maulana AmalNo ratings yet
- Migraine Hemicrania and Its Homeopathic Permanent Cure - DR Bashir Mahmud ElliasDocument7 pagesMigraine Hemicrania and Its Homeopathic Permanent Cure - DR Bashir Mahmud ElliasBashir Mahmud ElliasNo ratings yet
- Scally - Anabolic Steroids - A Question of MuscleDocument0 pagesScally - Anabolic Steroids - A Question of MuscleFabian MolinaNo ratings yet
- Drug StudyDocument14 pagesDrug StudyJho Ocampo NungayNo ratings yet
- Immunology Questions by DR TaherDocument26 pagesImmunology Questions by DR TaherChenthanKrishNo ratings yet
- Patent Ductus ArteriosusDocument48 pagesPatent Ductus ArteriosusPaul A IBattledaily ScavellaNo ratings yet
- ALS DietDocument36 pagesALS DietStemCellMDNo ratings yet
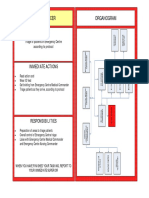
- Triage Officer Organogram: MissionDocument14 pagesTriage Officer Organogram: Missionsnow fazliNo ratings yet
- Syringe Final PresentationDocument30 pagesSyringe Final PresentationKhalid MahmoodNo ratings yet
- Anosognosia FSDocument2 pagesAnosognosia FSraquel perezNo ratings yet
- Peptic Ulcer DiseaseDocument3 pagesPeptic Ulcer DiseaseleahraizaNo ratings yet
- Department of Orthopaedic and Traumatology Faculty of Medicine - Hasanuddin University Makassar 2017Document24 pagesDepartment of Orthopaedic and Traumatology Faculty of Medicine - Hasanuddin University Makassar 2017aritrisnawatiNo ratings yet
- Transfusion Medicine Thesis TopicsDocument4 pagesTransfusion Medicine Thesis Topicsgjggsf72100% (2)
- Restricted Episiotomy and Perineal Repair: By: Surakshya Bhattarai WHD, MN 1 Year BHNC, Nams Roll No: 10Document70 pagesRestricted Episiotomy and Perineal Repair: By: Surakshya Bhattarai WHD, MN 1 Year BHNC, Nams Roll No: 10Surakshya BhattaraiNo ratings yet
- Tugas Efn II Unit 13Document4 pagesTugas Efn II Unit 13FransiscaapNo ratings yet
- National Insurance Company LimitedDocument6 pagesNational Insurance Company LimitedJeet MaruNo ratings yet
- Powerpoint Presentation On AIDSDocument27 pagesPowerpoint Presentation On AIDSChedan B. Ceriaco90% (20)
- 2010 Sofia Aroca SoteloDocument52 pages2010 Sofia Aroca SoteloAhmed BadrNo ratings yet
- Zoomrx - Data Science Case Study: BackgroundDocument2 pagesZoomrx - Data Science Case Study: Backgroundsudharsan_tkgNo ratings yet
- Paper 2Document12 pagesPaper 2Yeim Khay MoNo ratings yet
- Creationism EssayDocument5 pagesCreationism Essayd3gpmvqw100% (2)
- Topic 13 Global Distribution of Diseases My NC Notes 1Document31 pagesTopic 13 Global Distribution of Diseases My NC Notes 1Melogina ManoNo ratings yet
- Blood Urea Sampling Jul 2005Document6 pagesBlood Urea Sampling Jul 2005Handoko HalimNo ratings yet
- Drug Development: Basic: Phase I-III: Overview of Clinical TrialsDocument71 pagesDrug Development: Basic: Phase I-III: Overview of Clinical TrialsKomal KhanNo ratings yet
- Factors That Affect BMRDocument3 pagesFactors That Affect BMRNursakinah NajwahNo ratings yet
- White SlimeDocument4 pagesWhite SlimeSammyNo ratings yet
- Shortening of A Penrose DrainDocument2 pagesShortening of A Penrose DrainHeidi Avediz Del FuerteNo ratings yet
- Blush 2012 Acute Bronchitis PDFDocument7 pagesBlush 2012 Acute Bronchitis PDFMarimar FilardoNo ratings yet
- UreaDocument1 pageUreaDesiNo ratings yet