You might also like
- The Feeling of Meaninglessness: A Challenge To PsychotherapyDocument5 pagesThe Feeling of Meaninglessness: A Challenge To PsychotherapySwami Karunakarananda0% (1)
- Ocular TraumaDocument50 pagesOcular TraumafatimaNo ratings yet
- Ocular EmergencyDocument29 pagesOcular EmergencyMohammad Farouq Omar100% (3)
- Common Ocular EmergenciesDocument33 pagesCommon Ocular EmergenciesMaimoona AimanNo ratings yet
- K.15 Ophtalmologic EmergenciesDocument35 pagesK.15 Ophtalmologic EmergenciesZikri Putra Lan Lubis100% (1)
- Ocular Injuries and EmergenciesDocument60 pagesOcular Injuries and Emergenciesarnol3090100% (1)
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)
- Fluorescein AngiographyDocument81 pagesFluorescein Angiographyeng_25122147100% (4)
- Common Eye Problems and DiagnosisDocument84 pagesCommon Eye Problems and Diagnosisvivekrajbhilai5850No ratings yet
- Case Report Bacterial Conjunctivitis WengDocument9 pagesCase Report Bacterial Conjunctivitis WengIka NovitaNo ratings yet
- BlepharitisDocument11 pagesBlepharitismohamadNo ratings yet
- Fluorescein Angiography Basic Principles and InterpretationDocument58 pagesFluorescein Angiography Basic Principles and InterpretationAllaaeldin91% (11)
- Uveitis 140205125134 Phpapp02Document139 pagesUveitis 140205125134 Phpapp02ﻣﻠﻚ عيسىNo ratings yet
- TrabeculectomyDocument28 pagesTrabeculectomyAlfu RafdiNo ratings yet
- Eye ExamDocument12 pagesEye ExamQing Liang OngNo ratings yet
- Conjunctiva Anatomy and PhysiologyDocument106 pagesConjunctiva Anatomy and Physiologysaddam0% (1)
- Ocular Emergencies CMEDocument35 pagesOcular Emergencies CMEAmir Izzuddin SuibNo ratings yet
- What Is A Pinguecula and A PterygiumDocument5 pagesWhat Is A Pinguecula and A PterygiumandrewNo ratings yet
- Ophthalmology Revision LectureDocument80 pagesOphthalmology Revision LectureCarla LaniganNo ratings yet
- Drugs & Ophthalmology CCDocument16 pagesDrugs & Ophthalmology CCbahaashakirNo ratings yet
- Periorbital and Orbital CellulitisDocument51 pagesPeriorbital and Orbital CellulitisJoanne BlancoNo ratings yet
- Ophthalmologic Exam PDFDocument70 pagesOphthalmologic Exam PDFSamsam Almarez BacaltosNo ratings yet
- Classification of Ptosis: 1. NeurogenicDocument25 pagesClassification of Ptosis: 1. NeurogenicMuliany PratiwiNo ratings yet
- Anaesthesia For Cataract Surgery and Its ComplicationDocument28 pagesAnaesthesia For Cataract Surgery and Its Complicationbala16690No ratings yet
- Introduction To Low VisionDocument15 pagesIntroduction To Low VisionHira AtifNo ratings yet
- Choice of Artificial Tear Formulation For Patients With Dry Eye: Where Do We Start?Document5 pagesChoice of Artificial Tear Formulation For Patients With Dry Eye: Where Do We Start?Priscila Verduzco100% (1)
- Indirect OphthalmosDocument44 pagesIndirect Ophthalmosshar_s85No ratings yet
- Indirect OphthalmosDocument3 pagesIndirect Ophthalmosbijujc100% (1)
- School Eye Screening and The National Program For Control of Blindness - 2Document6 pagesSchool Eye Screening and The National Program For Control of Blindness - 2rendyjiwonoNo ratings yet
- Congenital Anomalies of UveaDocument16 pagesCongenital Anomalies of UveaHarika GuduruNo ratings yet
- Oculomotor NerveDocument4 pagesOculomotor NerveHuzaifah IbrahimNo ratings yet
- Ocular Manifestations of Thyroid DiseaseDocument20 pagesOcular Manifestations of Thyroid Diseasevivekrajbhilai5850No ratings yet
- Retinal Drawing A Lost Art of MedicineDocument3 pagesRetinal Drawing A Lost Art of MedicinekavyaNo ratings yet
- Corneal UlcerDocument21 pagesCorneal UlcerarturocerpaNo ratings yet
- Congenital CataractDocument40 pagesCongenital CataractRaymonde UyNo ratings yet
- Congnital CataractDocument44 pagesCongnital CataractMobile AsdNo ratings yet
- Case of A.D.G.: San Beda University - College of Medicine Bautista, Bayona, Boñula Ophthalmology RotationDocument18 pagesCase of A.D.G.: San Beda University - College of Medicine Bautista, Bayona, Boñula Ophthalmology RotationRonel MarkNo ratings yet
- Eyelid Lumps and BumpsDocument43 pagesEyelid Lumps and BumpsAbdul HannanNo ratings yet
- 4 TrachomaDocument27 pages4 TrachomaMarshet GeteNo ratings yet
- HyperopiaDocument6 pagesHyperopiaTesfsh MekonenNo ratings yet
- PterygiumDocument3 pagesPterygiumtri_budi_20No ratings yet
- Ophthalmology Final TransDocument51 pagesOphthalmology Final TransPatryk Dionisio100% (1)
- Non Mechanical and Chemical InjuriesDocument14 pagesNon Mechanical and Chemical InjuriesMuaz AbdullahNo ratings yet
- Hordeolum & ChalazionDocument22 pagesHordeolum & ChalazionDion Satriawan Dhaniardi100% (1)
- 1 - Ocular TraumaDocument31 pages1 - Ocular TraumadeoshiNo ratings yet
- Non-Concomitant Strabismus 2Document60 pagesNon-Concomitant Strabismus 2Ijeoma Okpalla100% (2)
- Types of Amblyopia - American Academy of OphthalmologyDocument1 pageTypes of Amblyopia - American Academy of OphthalmologyIraNo ratings yet
- RvoDocument43 pagesRvoOrchlon LkNo ratings yet
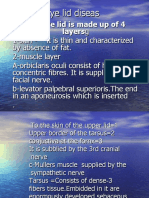
- Eye Lid DiseasDocument59 pagesEye Lid DiseasJohanna Tania PriatoNo ratings yet
- 13 Subjective RefractionDocument19 pages13 Subjective Refractionmuhammad farizNo ratings yet
- Optics and RefractionDocument12 pagesOptics and RefractionOscar Daniel MendezNo ratings yet
- Uveitis PDFDocument17 pagesUveitis PDFkmiz85No ratings yet
- 7.1 Gradual Loss of VisionDocument19 pages7.1 Gradual Loss of VisionparugandooNo ratings yet
- Primary Angle Closure GlaucomaDocument39 pagesPrimary Angle Closure GlaucomaMaria ShafiqNo ratings yet
- Corneal Ulcer: Prepared By: Renuka Shrestha Roll No: 29 PBBN 3rd Year SMTCDocument41 pagesCorneal Ulcer: Prepared By: Renuka Shrestha Roll No: 29 PBBN 3rd Year SMTCsushma shresthaNo ratings yet
- Examination of Eye PT IIDocument77 pagesExamination of Eye PT IIMihaela TomaNo ratings yet
- Racgp Floaters and Flashes OpthalmologyDocument3 pagesRacgp Floaters and Flashes OpthalmologyBeaulah HunidzariraNo ratings yet
- Infectious Keratitis Final PDFDocument99 pagesInfectious Keratitis Final PDFGetenet shumetNo ratings yet
- NATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideFrom EverandNATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideNo ratings yet
- Scientific Foundations of OphthalmologyFrom EverandScientific Foundations of OphthalmologyEdward S. PerkinsNo ratings yet
- Complications of Thoracic SurgeryDocument45 pagesComplications of Thoracic SurgeryAlin ToaderNo ratings yet
- Batch IVDocument28 pagesBatch IVRizqy DwitamaNo ratings yet
- Appendicitis Case StudyDocument2 pagesAppendicitis Case StudyLeviThomasStafford100% (1)
- Mental Health Resources For The Asian American CommunityDocument4 pagesMental Health Resources For The Asian American CommunitydisgrasianNo ratings yet
- Pathology Clinic Nasopharyngeal CarcinomaDocument2 pagesPathology Clinic Nasopharyngeal CarcinomaTukang Gali KuburNo ratings yet
- Generic Modified Release Drug ProductsDocument43 pagesGeneric Modified Release Drug ProductsShilpa Kotian100% (1)
- Pcos GP Tool 2dec2013Document6 pagesPcos GP Tool 2dec2013Maram AbdullahNo ratings yet
- Sexually Connotative Disorders - ScribdDocument18 pagesSexually Connotative Disorders - ScribdMae AzoresNo ratings yet
- Disorders of HemostasisDocument50 pagesDisorders of Hemostasisalibayaty1100% (1)
- Comparison of Bipolar and Monopolar Cautry Use in Turp For Treatment of Enlarged ProstateDocument4 pagesComparison of Bipolar and Monopolar Cautry Use in Turp For Treatment of Enlarged ProstatebreadfanNo ratings yet
- Lapitan NCP MyelomeningoceleDocument4 pagesLapitan NCP MyelomeningoceleRea LapitanNo ratings yet
- Casediscussion Ludwig's Angina Review PDFDocument5 pagesCasediscussion Ludwig's Angina Review PDFBima BaskaraNo ratings yet
- Patellar FractureDocument25 pagesPatellar FractureSyafiq ShahbudinNo ratings yet
- Handicap International - HaitiDocument18 pagesHandicap International - HaitiInterActionNo ratings yet
- Community PsychologyDocument20 pagesCommunity PsychologyMaePornelaGomezNo ratings yet
- Fibrous Dysplasia: A ReviewDocument5 pagesFibrous Dysplasia: A ReviewJuhiJahan AmanullahNo ratings yet
- Evolution of The Sensory Integration Frame of ReferenceDocument5 pagesEvolution of The Sensory Integration Frame of ReferenceBranislava Jaranovic VujicNo ratings yet
- Acupressure Training Course: Synopsis of Lesson IDocument2 pagesAcupressure Training Course: Synopsis of Lesson IAshishNo ratings yet
- 201.controlled Release Oral Drug Delivery SystemDocument35 pages201.controlled Release Oral Drug Delivery SystemRajesh Akki0% (1)
- Psychology - Article 38Document1 pagePsychology - Article 38piping stressNo ratings yet
- Apriladi Hypnosis For Cancer A Hypnotists Guide To Helping Those in NeedDocument13 pagesApriladi Hypnosis For Cancer A Hypnotists Guide To Helping Those in NeedApriladi Putra Pegagan100% (2)
- Gardasil VAERS Adverse ReactionsDocument1,824 pagesGardasil VAERS Adverse Reactionsmcdonald.rr100% (2)
- DYHFS10 Cancer Prevention Mar 2005Document2 pagesDYHFS10 Cancer Prevention Mar 2005Ngaire TaylorNo ratings yet
- Career Shadowing PTDocument3 pagesCareer Shadowing PTapi-703338120No ratings yet
- Chapter 22Document6 pagesChapter 22Danielle ShullNo ratings yet
- Bipolar DisorderDocument10 pagesBipolar DisorderJimmy100% (1)
- First Generation Antipsychotic Agents / Neuroleptics 1Document4 pagesFirst Generation Antipsychotic Agents / Neuroleptics 1Brylle ArbasNo ratings yet
- Ernest Rossi Mind Body PsychotherapyDocument8 pagesErnest Rossi Mind Body PsychotherapyFernandoNo ratings yet
- Pocket Tutor Understanding ABGs and Lung Function TestsDocument170 pagesPocket Tutor Understanding ABGs and Lung Function Testsdanelv100% (1)