You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lulu Hasna - PPT Journal Reading AnesthesiaDocument11 pagesLulu Hasna - PPT Journal Reading AnesthesiaMaya PermataNo ratings yet
- Rajasthan Power Utility Pensioners to Get Medical Benefits Only at Approved HospitalsDocument7 pagesRajasthan Power Utility Pensioners to Get Medical Benefits Only at Approved HospitalsTaresh MittalNo ratings yet
- Health History and AssessmentDocument2 pagesHealth History and AssessmentRalph Justin Tongos100% (1)
- CT Bowel Wall ThickeningDocument14 pagesCT Bowel Wall ThickeningAjeetalbertNo ratings yet
- Hemostatic and Thrombotic Considerations in The Diagnosis and ManagementDocument12 pagesHemostatic and Thrombotic Considerations in The Diagnosis and Managementender izaguirreNo ratings yet
- 2024 USFSSTG001V4 US DeLorean STG Rev1aDocument70 pages2024 USFSSTG001V4 US DeLorean STG Rev1aNathaly GuevaraNo ratings yet
- Bleeding During PregnancyDocument5 pagesBleeding During PregnancyMaryela Maceda GalozoNo ratings yet
- Suffixes and PrefixesDocument8 pagesSuffixes and PrefixesMaya ElenaNo ratings yet
- NGT InsertionDocument1 pageNGT InsertionNURSES' PAD100% (3)
- Multiple-Choice Questionnaire: Functional Pelvic Floor ImagingDocument3 pagesMultiple-Choice Questionnaire: Functional Pelvic Floor Imagingtesfaye mekonnenNo ratings yet
- Role of Multi Detector (MDCT)Document52 pagesRole of Multi Detector (MDCT)ramon100% (5)
- Initial Assessment & Management Polytrauma: July 4, 2015 1Document54 pagesInitial Assessment & Management Polytrauma: July 4, 2015 1parkmickybooNo ratings yet
- Second Announcement PERAPIDocument12 pagesSecond Announcement PERAPIizzah awwalinNo ratings yet
- 2CreditTest TerminologyDocument26 pages2CreditTest TerminologyAna Carballo TrabazoNo ratings yet
- Iliac CrestDocument32 pagesIliac CrestDR NASIMNo ratings yet
- Emergency Drug Box Approved ListDocument1 pageEmergency Drug Box Approved ListGee_anne_Saldi_9627No ratings yet
- Kelaidi Catalogue - Medical EquipmentDocument13 pagesKelaidi Catalogue - Medical EquipmentEmmanuel Siyansima MwaseNo ratings yet
- A Postgraduate Seminar On Shock CorrectedDocument69 pagesA Postgraduate Seminar On Shock Correctedboma georgeNo ratings yet
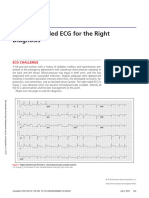
- 2018.the Right-Sided ECG For The Right DiagnosisDocument3 pages2018.the Right-Sided ECG For The Right DiagnosisWeila dos Santos VieiraNo ratings yet
- Robotic Surgery History and SystemsDocument28 pagesRobotic Surgery History and SystemsLidhi DileepNo ratings yet
- DR Luca Vricella Interview Transcript 1Document19 pagesDR Luca Vricella Interview Transcript 1api-690757487No ratings yet
- Pengalaman Menjalani Hemodialisa Pada Pasien Gagal Ginjal KronisDocument10 pagesPengalaman Menjalani Hemodialisa Pada Pasien Gagal Ginjal KronisTien KartiniNo ratings yet
- Uptodate: Chronic Kidney DiseaseDocument13 pagesUptodate: Chronic Kidney DiseaseAtiqah ShahNo ratings yet
- ECG Nutshell - Beta Free VersionDocument24 pagesECG Nutshell - Beta Free Versionnaveen prasanthNo ratings yet
- 2021JULYDocument25 pages2021JULYNicole VinnikNo ratings yet
- Deena Horn DPM AACFAS, John Doolan DPM FACFAS, Adam Cirlincione FACFAS DPM Joseph Larsen DPM FACFASDocument1 pageDeena Horn DPM AACFAS, John Doolan DPM FACFAS, Adam Cirlincione FACFAS DPM Joseph Larsen DPM FACFASbaoNo ratings yet
- Discharge SummaryDocument3 pagesDischarge SummaryMuhammad KhudriNo ratings yet
- Multiple Choice Questions (MCQS) in Anatomy-General Anatomy & Upper LimbDocument10 pagesMultiple Choice Questions (MCQS) in Anatomy-General Anatomy & Upper LimbLoisNo ratings yet
- Surgical Site MarkingDocument16 pagesSurgical Site Markingalejandrino_leoaugustoNo ratings yet
- Near Misses in Cardiac Surgery Second EditionDocument189 pagesNear Misses in Cardiac Surgery Second EditionAfnan MoeNo ratings yet