You might also like
- Step 2ck Important (AutoRecovered)Document101 pagesStep 2ck Important (AutoRecovered)Aishwarya SridharNo ratings yet
- Detecting The Differences Radiculopathy, Myelopathy and Peripheral NeuropathyDocument70 pagesDetecting The Differences Radiculopathy, Myelopathy and Peripheral Neuropathyapi-19502000100% (8)
- Practice Essentials: Essential Update: Chemotherapy Following Radiation May Improve Survival in Low-Grade GliomasDocument19 pagesPractice Essentials: Essential Update: Chemotherapy Following Radiation May Improve Survival in Low-Grade GliomasFika Khulma SofiaNo ratings yet
- Psychiatry PasTest MRCP II 2019Document71 pagesPsychiatry PasTest MRCP II 2019jehemirNo ratings yet
- C Spine Clearance Ortho 3 Journal ClubDocument31 pagesC Spine Clearance Ortho 3 Journal ClubMuvenn KannanNo ratings yet
- Oesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHDocument50 pagesOesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHMalgh Kh100% (2)
- Beasts of The Earth Animals, Humans, and DiseaseDocument206 pagesBeasts of The Earth Animals, Humans, and Diseasehadrian75100% (1)
- Malignant Spinal Cord Compression - Dealing The Most Common - MetsDocument60 pagesMalignant Spinal Cord Compression - Dealing The Most Common - MetsDr Sasikumar Sambasivam100% (2)
- Measurements in EpidemiologyDocument24 pagesMeasurements in EpidemiologyAnand gowda75% (4)
- Meralgia ParestheticaDocument22 pagesMeralgia ParestheticaWahyu Tri KusprasetyoNo ratings yet
- Acute Bronchitis Case StudyDocument6 pagesAcute Bronchitis Case Studyulka0750% (2)
- Endocrine Surgery MCQDocument71 pagesEndocrine Surgery MCQShriyansh ChaharNo ratings yet
- Emergency in OncologiDocument70 pagesEmergency in OncologiAzwin KamarNo ratings yet
- Tuberculous Spondylitis (TB Spine/pott's Disease)Document28 pagesTuberculous Spondylitis (TB Spine/pott's Disease)Divo Septian Zarwin100% (1)
- Pancreatic CancerDocument4 pagesPancreatic Cancersdf100% (1)
- ATLS Post TestDocument1 pageATLS Post Testanon_57896987836% (56)
- Nursing Care Plan "Diabetes"Document8 pagesNursing Care Plan "Diabetes"Senor SeniorNo ratings yet
- Health Research Fundamentals - EnglishDocument380 pagesHealth Research Fundamentals - EnglishRamNo ratings yet
- Tuberculosis Spondylitis IIDocument40 pagesTuberculosis Spondylitis IICendraiin MinangkabauNo ratings yet
- International Health RegulationDocument60 pagesInternational Health RegulationAnonymous 7ugfwjsHQUNo ratings yet
- Nursing in Chirurgie GeneralaDocument64 pagesNursing in Chirurgie GeneralaChiperi CristinaNo ratings yet
- Rehabilitation and Treatment of Spinal Cord TumorsDocument8 pagesRehabilitation and Treatment of Spinal Cord TumorsAndreea SlabuNo ratings yet
- Spinal Cord Tumours: Mr. ANILKUMAR B R (MS.C Nursing) Lecturer, Medical-Surgical NursingDocument24 pagesSpinal Cord Tumours: Mr. ANILKUMAR B R (MS.C Nursing) Lecturer, Medical-Surgical NursingElfa AlfiyaniNo ratings yet
- Degenerative Disc Disease by Dr. BBTDocument11 pagesDegenerative Disc Disease by Dr. BBTBhusan TamrakarNo ratings yet
- Purpose: Grading of The Neurological DeficitDocument28 pagesPurpose: Grading of The Neurological DeficitAkbar Kapissa BaharsyahNo ratings yet
- Spinal Infections: Khoirunnisa Humairoh (702016075)Document31 pagesSpinal Infections: Khoirunnisa Humairoh (702016075)Khoirunnisa HumairohNo ratings yet
- Leukemia and Lymphoma Metastases: Lisa M. D AngelisDocument13 pagesLeukemia and Lymphoma Metastases: Lisa M. D AngelisjaquelineartNo ratings yet
- (10920684 - Neurosurgical Focus) Intramedullary Spinal Cord Tumors - A Review of Current and Future Treatment StrategiesDocument10 pages(10920684 - Neurosurgical Focus) Intramedullary Spinal Cord Tumors - A Review of Current and Future Treatment StrategiesSachin RajaNo ratings yet
- Childhood Malignancies PP - Copy 2Document46 pagesChildhood Malignancies PP - Copy 2ugonna nwokeNo ratings yet
- Tuberculosis of Spine: Current Views in Diagnosis and ManagementDocument13 pagesTuberculosis of Spine: Current Views in Diagnosis and ManagementNurul HidayahNo ratings yet
- Spinal Infections: Khoirunnisa Humairoh (702016075)Document31 pagesSpinal Infections: Khoirunnisa Humairoh (702016075)Khoirunnisa HumairohNo ratings yet
- Slkdmsalkdmla Sa NlasDocument12 pagesSlkdmsalkdmla Sa NlasjdjhdNo ratings yet
- Spinal Tumor: Zelin Sun MD, PH.DDocument28 pagesSpinal Tumor: Zelin Sun MD, PH.DMargaret ThatcherNo ratings yet
- Surgery Imp QuestionsDocument29 pagesSurgery Imp Questionsakshit bhambriNo ratings yet
- Two Content Layout With Table: Common Pediatric MalignanciesDocument34 pagesTwo Content Layout With Table: Common Pediatric MalignanciesnazymalfikryNo ratings yet
- Acute Back PainDocument6 pagesAcute Back PainWahyudi TriNo ratings yet
- On Co EmergenciesDocument6 pagesOn Co EmergenciessdfNo ratings yet
- Pituitary TumorsDocument6 pagesPituitary Tumorsapi-271668042No ratings yet
- Practice Essentials: Signs and SymptomsDocument20 pagesPractice Essentials: Signs and SymptomsrainbowshopNo ratings yet
- Pott's Disease MEDICAL MANAGEMENTDocument3 pagesPott's Disease MEDICAL MANAGEMENTRuby Anna BorceNo ratings yet
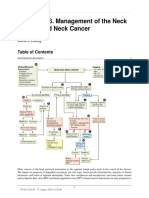
- Chapter 146. Management of The Neck in Head and Neck Cancer: David E EiblingDocument3 pagesChapter 146. Management of The Neck in Head and Neck Cancer: David E EiblingYasin KulaksızNo ratings yet
- Herniated Nucleus Pulposus TreatmentDocument19 pagesHerniated Nucleus Pulposus Treatmentvicky174No ratings yet
- Enocrine Surgery MCQDocument56 pagesEnocrine Surgery MCQlana792010No ratings yet
- Radiculopatia CervicalDocument8 pagesRadiculopatia CervicalFACIVERINo ratings yet
- Continuing Education ActivityDocument3 pagesContinuing Education ActivityMuhammad Waris HarganNo ratings yet
- Neck Pain and Lower Back Pain. Med Clin N Am. 2019.Document14 pagesNeck Pain and Lower Back Pain. Med Clin N Am. 2019.Jose Fernando Diez100% (1)
- 0-306-48407-2 - 35 - 2023-02-23T214346.871Document13 pages0-306-48407-2 - 35 - 2023-02-23T214346.871drsubramanianNo ratings yet
- Sem5 Protocol SCCDocument20 pagesSem5 Protocol SCCOlga Manco GuzmánNo ratings yet
- Brain TumorsDocument11 pagesBrain TumorsAmmar Bin KhalilNo ratings yet
- Spine Metastasis Dari MedscapeDocument15 pagesSpine Metastasis Dari MedscapeZakiyul FuadNo ratings yet
- Spinal Cord CompressionDocument7 pagesSpinal Cord CompressionMarius Clifford BilledoNo ratings yet
- CEE Based Question and Answer Asar 30 080Document74 pagesCEE Based Question and Answer Asar 30 080aayam adhikariNo ratings yet
- Ca Nasofaring - NanaDocument26 pagesCa Nasofaring - Nananovias_4No ratings yet
- Urinary Tract CancerDocument53 pagesUrinary Tract CancerandikaisnaeniNo ratings yet
- Sem5 - Spinal Cord CompressionDocument11 pagesSem5 - Spinal Cord CompressionOlga Manco GuzmánNo ratings yet
- Tuberculosis of SpineDocument19 pagesTuberculosis of SpinemelittaaNo ratings yet
- Cancer, Nasopharyngeal Carcinoma (NPC) : Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2020 JanDocument11 pagesCancer, Nasopharyngeal Carcinoma (NPC) : Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2020 JanikaNo ratings yet
- Understanding Medical Surgical Nursing - 0835-0835Document1 pageUnderstanding Medical Surgical Nursing - 0835-0835Anas TasyaNo ratings yet
- CNS PBL 2Document6 pagesCNS PBL 2Hugh JacobsNo ratings yet
- Cervical Spondylotic Myelopathy: Aditya Iyer, MD, MS, Tej D. Azad, Ba, and Suzanne Tharin, MD, PHDDocument7 pagesCervical Spondylotic Myelopathy: Aditya Iyer, MD, MS, Tej D. Azad, Ba, and Suzanne Tharin, MD, PHDMây Trên TrờiNo ratings yet
- Oncologic or Degenerative Neurologic DisordersDocument15 pagesOncologic or Degenerative Neurologic DisordersDinarkram Rabreca EculNo ratings yet
- Current Approach To Obstetric Brachial Plexus Palsy (#127683) - 109205 SCOLIOSIS SecuelasDocument7 pagesCurrent Approach To Obstetric Brachial Plexus Palsy (#127683) - 109205 SCOLIOSIS SecuelaswilhelmNo ratings yet
- Meningioma in The Lumbar SpineDocument12 pagesMeningioma in The Lumbar Spinemex487No ratings yet
- Radiology PearlsDocument2 pagesRadiology PearlsSalman Rashid100% (2)
- Solid TumoursDocument48 pagesSolid TumoursViswanadh BNo ratings yet
- Metastatic Spinal Cord Compression: A Rare But Important Complication of CancerDocument4 pagesMetastatic Spinal Cord Compression: A Rare But Important Complication of CancerDhila ThasliyahNo ratings yet
- Renal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaDocument5 pagesRenal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaMohamed Al-zichrawyNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- FAB Classification of ALLDocument4 pagesFAB Classification of ALLjehemirNo ratings yet
- Bone Marrow Compartmetn by MohsenDocument6 pagesBone Marrow Compartmetn by MohsenjehemirNo ratings yet
- 4 521174069253505140Document8 pages4 521174069253505140jehemirNo ratings yet
- Ovaries CancerDocument29 pagesOvaries CancerjehemirNo ratings yet
- Febrile Neutropenia: Dr. Abdelkareem Wedaa EltohamyDocument31 pagesFebrile Neutropenia: Dr. Abdelkareem Wedaa Eltohamyjehemir100% (1)
- What Do You Need To Know About Breast Cancer: DR / Mokhtar Gusmallah Clinical OncologistDocument26 pagesWhat Do You Need To Know About Breast Cancer: DR / Mokhtar Gusmallah Clinical OncologistjehemirNo ratings yet
- Ophthalmology For The Equine Practitioner 2002-2002Document2 pagesOphthalmology For The Equine Practitioner 2002-2002Francisco JulianNo ratings yet
- Concept PaperDocument1 pageConcept PaperKurt NicolasNo ratings yet
- The Correlation of Self Efficacy With Coping Strategies On Patients Diabetes Mellitus Type 2 Which Use Insulin in Waled Hospital of Cirebon DistrictDocument7 pagesThe Correlation of Self Efficacy With Coping Strategies On Patients Diabetes Mellitus Type 2 Which Use Insulin in Waled Hospital of Cirebon DistrictSyarief NurseNo ratings yet
- Parent Letter Choking GameDocument2 pagesParent Letter Choking GameU.s. Africa CommandNo ratings yet
- Dengue PreventionDocument8 pagesDengue PreventionqetaNo ratings yet
- ICD 10 CM Official Coding Gudance Interim Advice Coronavirus Feb 20 2020 PDFDocument3 pagesICD 10 CM Official Coding Gudance Interim Advice Coronavirus Feb 20 2020 PDFSumiwaty PanNo ratings yet
- EDITORIAL Successful Treatment Strategy of Turkey Against Covid19 Outbreak-12345 PDFDocument2 pagesEDITORIAL Successful Treatment Strategy of Turkey Against Covid19 Outbreak-12345 PDFMohaymin AljabryNo ratings yet
- NeuroblastomaDocument21 pagesNeuroblastomaRichard DjigoNo ratings yet
- Gambaran Usia Pada Kejadian Covid-19: Rosyada Elviani Chairil Anwar Rico Januar SitorusDocument6 pagesGambaran Usia Pada Kejadian Covid-19: Rosyada Elviani Chairil Anwar Rico Januar SitorusRizka ZahroNo ratings yet
- CystitisDocument10 pagesCystitisJeffNo ratings yet
- 10.3 - Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value - STAT 507Document3 pages10.3 - Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value - STAT 507Avinash sahu100% (1)
- Covid Vaccine CertificateDocument1 pageCovid Vaccine CertificateSahil KurudeNo ratings yet
- Baby Massage Consultation Form - November 2017Document1 pageBaby Massage Consultation Form - November 2017api-257327106No ratings yet
- Health Assessment (Eye, Ear, Mouth, Throat, Nose and Sinuses)Document5 pagesHealth Assessment (Eye, Ear, Mouth, Throat, Nose and Sinuses)Tricia Joy EspinosaNo ratings yet
- Mengurangkan Penularan Wabak Influenza AH1N1 Di Institusi Dan SekolahDocument31 pagesMengurangkan Penularan Wabak Influenza AH1N1 Di Institusi Dan Sekolahts0104No ratings yet
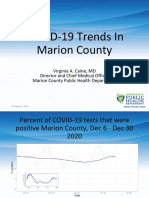
- Marion County Public Health Update 01.07.21Document15 pagesMarion County Public Health Update 01.07.21Last DayNo ratings yet
- Malaria in Pregnancy. NewDocument23 pagesMalaria in Pregnancy. Newgloriashirima8No ratings yet
- HIV in Children: Preventing Mother-to-Child Transmission (Dr. Laura Guay)Document27 pagesHIV in Children: Preventing Mother-to-Child Transmission (Dr. Laura Guay)National Press FoundationNo ratings yet
- Vis RabiesDocument2 pagesVis RabiesSanjay KumarNo ratings yet
- Fleischner Society Guideline PDFDocument14 pagesFleischner Society Guideline PDFBiswarup PurkayasthaNo ratings yet
- Indonesia Health SectorDocument84 pagesIndonesia Health SectorBung RandiNo ratings yet
- Ulcerative ColitisDocument15 pagesUlcerative Colitisapi-252717471100% (1)