You might also like
- Comprehensive: Geriatric AssessmentDocument38 pagesComprehensive: Geriatric AssessmentDingsNo ratings yet
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionFrom EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionNo ratings yet
- 8 Common Charting Mistakes To Avoi1aDocument4 pages8 Common Charting Mistakes To Avoi1aEggy PascualNo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- IE - Antibiotic TableDocument5 pagesIE - Antibiotic TablemeganNo ratings yet
- Cerebrovascular Ultrasound in Stroke Prevention and TreatmentFrom EverandCerebrovascular Ultrasound in Stroke Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- Fast Facts: Kidney Itch: CKD-associated pruritus: under-recognized and under-treatedFrom EverandFast Facts: Kidney Itch: CKD-associated pruritus: under-recognized and under-treatedNo ratings yet
- Human Tumours Secreting Catecholamines: Clinical and Physiopathological Study of the PheochromocytomasFrom EverandHuman Tumours Secreting Catecholamines: Clinical and Physiopathological Study of the PheochromocytomasRating: 5 out of 5 stars5/5 (1)
- Diagnostic Electron Microscopy: A Practical Guide to Interpretation and TechniqueFrom EverandDiagnostic Electron Microscopy: A Practical Guide to Interpretation and TechniqueNo ratings yet
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Palliative EnciesDocument96 pagesPalliative EnciesnandanNo ratings yet
- Diabetes Management in Long-Term Settings: A Clinician's Guide to Optimal Care for the ElderlyFrom EverandDiabetes Management in Long-Term Settings: A Clinician's Guide to Optimal Care for the ElderlyNo ratings yet
- Final 2010 GYN Module Clinical ObjectivesDocument36 pagesFinal 2010 GYN Module Clinical Objectiveslolapell100% (1)
- Cognitive Disorders Due to Medical ConditionsDocument18 pagesCognitive Disorders Due to Medical ConditionsSri HazizahNo ratings yet
- Preventive Health: Based On The USPSTF 2014Document42 pagesPreventive Health: Based On The USPSTF 2014Louella CarpioNo ratings yet
- CCJM Symptom Management An Important Part of Cancer CareDocument10 pagesCCJM Symptom Management An Important Part of Cancer CareBrian HarrisNo ratings yet
- 2016 ASCO - ONS Chemo Standards PDFDocument13 pages2016 ASCO - ONS Chemo Standards PDFSindu SaiNo ratings yet
- Akd & CKDDocument44 pagesAkd & CKDﻣﻠﻚ عيسىNo ratings yet
- LECTURE 1 Introduction of InfectionDocument29 pagesLECTURE 1 Introduction of Infectiontari riyastiNo ratings yet
- Best Practice Recommendations For Holistic Strategies To Promote and Maintain Skin IntegrityDocument32 pagesBest Practice Recommendations For Holistic Strategies To Promote and Maintain Skin IntegrityisaNo ratings yet
- Evaluation of Liver FunctionDocument64 pagesEvaluation of Liver FunctionMustafa KhandgawiNo ratings yet
- Nephrology: Omar K MRCP IrelandDocument54 pagesNephrology: Omar K MRCP IrelandManmeet SNo ratings yet
- Assessing and Preventing Delirium in Hospitalized PatientsDocument34 pagesAssessing and Preventing Delirium in Hospitalized PatientsVishala MishraNo ratings yet
- Intradialytic Hypertension Time To Act 10Document7 pagesIntradialytic Hypertension Time To Act 10Nia FirdiantyNo ratings yet
- DeliriumDocument27 pagesDeliriumBushra EjazNo ratings yet
- Diabetes and Complications: When Documenting Diabetes, It's Important To Note The FollowingDocument2 pagesDiabetes and Complications: When Documenting Diabetes, It's Important To Note The Followingmeikaizen100% (1)
- Comprehensive Geriatric Assessment - UpToDateDocument41 pagesComprehensive Geriatric Assessment - UpToDateOvidiu-Lucian BajenaruNo ratings yet
- Justify Your DiagnosisDocument2 pagesJustify Your DiagnosisdrichgregoryNo ratings yet
- Diabetic Nephropathy: Assisstant Professor Dr. Mihaela-Dora DonciuDocument65 pagesDiabetic Nephropathy: Assisstant Professor Dr. Mihaela-Dora DonciuFloreaAndreiNo ratings yet
- Delirium Pathway - OTLPCM002-3Document1 pageDelirium Pathway - OTLPCM002-3Iftida YatiNo ratings yet
- Seizures in Children JULIO 2020Document29 pagesSeizures in Children JULIO 2020Elizabeth HendersonNo ratings yet
- Sleep Disorders in Children and Adolescents: Understanding Causes and Treatment OptionsDocument50 pagesSleep Disorders in Children and Adolescents: Understanding Causes and Treatment OptionsCitra Sukri Sugesti100% (1)
- Clinical Features of Renal DiseaseDocument80 pagesClinical Features of Renal DiseaseIdiAmadouNo ratings yet
- Anti-Anginal DrugsDocument39 pagesAnti-Anginal Drugspoonam rana100% (1)
- Ascites: Darien Liew DaojuinDocument28 pagesAscites: Darien Liew DaojuinDarien LiewNo ratings yet
- Case 36 AscitesDocument4 pagesCase 36 AscitesMichaelNo ratings yet
- Lodhi - Granulomatous Mastitis Docx Power Point2Document36 pagesLodhi - Granulomatous Mastitis Docx Power Point2Sehrish Siddique100% (1)
- Drug Cards For Aricept, Synthyroid, Flomax, Klor-Con M, Diphenoxylate-AtropineDocument3 pagesDrug Cards For Aricept, Synthyroid, Flomax, Klor-Con M, Diphenoxylate-AtropinemynursingtoolsNo ratings yet
- Yale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1Document12 pagesYale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1omegasauron0gmailcomNo ratings yet
- Tennessee Medicaid Claimed Hundreds of Millions of Federal Funds For Certified Public Expenditures That Were Not in Compliance With Federal RequirementsDocument36 pagesTennessee Medicaid Claimed Hundreds of Millions of Federal Funds For Certified Public Expenditures That Were Not in Compliance With Federal RequirementsFOX 17 NewsNo ratings yet
- Degenerative Joint DiseaseDocument35 pagesDegenerative Joint DiseaseWendy EscalanteNo ratings yet
- Nursing Home Other Long Term ServicesDocument44 pagesNursing Home Other Long Term ServicesHelloNo ratings yet
- KDIGO Guideline for Diagnosis and Treatment of CKD-MBDDocument65 pagesKDIGO Guideline for Diagnosis and Treatment of CKD-MBDCitra DessyNo ratings yet
- Renovascular Hypertension (RVH) SeminarDocument58 pagesRenovascular Hypertension (RVH) SeminarfaizalmasoodiNo ratings yet
- Ipdi NutrisiDocument53 pagesIpdi NutrisiDefan Dapat Titik TerangNo ratings yet
- Nclex Study GuideDocument37 pagesNclex Study GuideBlas Christian Tancongco ChavesNo ratings yet
- Blood Count Interpretation 1Document49 pagesBlood Count Interpretation 1ripangaNo ratings yet
- Cholangiocarcinoma: The Right Clinical Information, Right Where It's NeededDocument40 pagesCholangiocarcinoma: The Right Clinical Information, Right Where It's NeededHan KethyanethNo ratings yet
- ICU-Procedural 1st YearDocument3 pagesICU-Procedural 1st YearNephrology On-DemandNo ratings yet
- Disorders of Calcium and Phosphate MetabolismDocument20 pagesDisorders of Calcium and Phosphate MetabolismAhmed Noureldin AhmedNo ratings yet
- Physician & Dialysis - Economics Matters: Umesh KhannaDocument3 pagesPhysician & Dialysis - Economics Matters: Umesh Khannaunfriendly.gy2268No ratings yet
- Calcium Metabolism PraveenDocument42 pagesCalcium Metabolism PraveenDr PraveenNo ratings yet
- CC and MCC List For DRG CodingDocument1 pageCC and MCC List For DRG Codinge-MedTools100% (2)
- Chemotherapy Medicines for Breast Cancer TreatmentDocument2 pagesChemotherapy Medicines for Breast Cancer Treatmentr_mckenrick0% (1)
- Behavioral and Psychological Symptoms of Dementia (BPSDDocument17 pagesBehavioral and Psychological Symptoms of Dementia (BPSDChachaNo ratings yet
- Introduction, Lnstrumentation, Technique, Normal Sonoanatomy of MSK StructuresDocument33 pagesIntroduction, Lnstrumentation, Technique, Normal Sonoanatomy of MSK StructuresNurrahmanita AzizaNo ratings yet
- Determinant and Impact Fatigue in COPD 2009Document8 pagesDeterminant and Impact Fatigue in COPD 2009Nurrahmanita AzizaNo ratings yet
- Cognitive Function in COPDDocument10 pagesCognitive Function in COPDNurrahmanita AzizaNo ratings yet
- An Overview of Pathophysiology Assessment and Management StrategDocument8 pagesAn Overview of Pathophysiology Assessment and Management StrategNurrahmanita AzizaNo ratings yet
- Jenny AOS Review NeurocaseDocument7 pagesJenny AOS Review NeurocaseSebastián Contreras CubillosNo ratings yet
- Pre-Frailty and Risk of CVD in Elderly Men and Women PDFDocument8 pagesPre-Frailty and Risk of CVD in Elderly Men and Women PDFNurrahmanita AzizaNo ratings yet
- Research on Comparisons between Sabah and Diesel CyclesDocument8 pagesResearch on Comparisons between Sabah and Diesel CyclesjorgeNo ratings yet
- TLM4ALL@1 Number System (EM)Document32 pagesTLM4ALL@1 Number System (EM)jkc collegeNo ratings yet
- 6 An Indian American Woman in Space 2Document11 pages6 An Indian American Woman in Space 2Manju YadavNo ratings yet
- The Completely Randomized Design (CRD)Document16 pagesThe Completely Randomized Design (CRD)Rahul TripathiNo ratings yet
- HFH ch04Document11 pagesHFH ch04Harikrishan RNo ratings yet
- Medication Calculation Examination Study Guide: IV CalculationsDocument2 pagesMedication Calculation Examination Study Guide: IV Calculationswaqas_xsNo ratings yet
- Hotel Engineering Facilities: A Case Study of Maintenance PerformanceDocument7 pagesHotel Engineering Facilities: A Case Study of Maintenance PerformanceHoh Pui KeiNo ratings yet
- Amazon Invoice Books 4Document1 pageAmazon Invoice Books 4raghuveer9303No ratings yet
- BC Sample Paper-3Document4 pagesBC Sample Paper-3Roshini ANo ratings yet
- 02 1 Cohen Sutherland PDFDocument3 pages02 1 Cohen Sutherland PDFSarra AnitaNo ratings yet
- MCQs on PharmacologyDocument101 pagesMCQs on PharmacologyMohammad Rashid88% (8)
- Hunk 150Document2 pagesHunk 150Brayan Torres04No ratings yet
- Inventario de Autoestima de Coopersmith PDFDocument10 pagesInventario de Autoestima de Coopersmith PDFNancy BerduzcoNo ratings yet
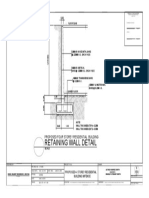
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet
- Training Report On Machine LearningDocument27 pagesTraining Report On Machine LearningBhavesh yadavNo ratings yet
- MINTZBERGDocument32 pagesMINTZBERGgeezee10004464100% (2)
- Fisher - Techincal Monograph 42 - Understanding DecibelsDocument8 pagesFisher - Techincal Monograph 42 - Understanding Decibelsleslie.lp2003No ratings yet
- Theory and Practice of Crown and Bridge Prosthodontics 4nbsped CompressDocument1,076 pagesTheory and Practice of Crown and Bridge Prosthodontics 4nbsped CompressYuganya SriNo ratings yet
- Sato Printer Api Reference DocumentDocument34 pagesSato Printer Api Reference Documentsupersteel.krwNo ratings yet
- My Watch Runs WildDocument3 pagesMy Watch Runs WildLarissa SnozovaNo ratings yet
- 0520 Int OTG P4 MSDocument12 pages0520 Int OTG P4 MSTrévina JosephNo ratings yet
- Cheat Codes SkyrimDocument13 pagesCheat Codes SkyrimDerry RahmaNo ratings yet
- KJR 20 880 PDFDocument14 pagesKJR 20 880 PDFNam LeNo ratings yet
- COR2-03 Admist The Mists and Coldest Frost PDFDocument16 pagesCOR2-03 Admist The Mists and Coldest Frost PDFLouis BachNo ratings yet
- Is Iso 2692-1992Document24 pagesIs Iso 2692-1992mwasicNo ratings yet
- Unit 7 Noun ClauseDocument101 pagesUnit 7 Noun ClauseMs. Yvonne Campbell0% (1)
- Chapter 25 (10) Capital Investment Analysis: ObjectivesDocument40 pagesChapter 25 (10) Capital Investment Analysis: ObjectivesJames BarzoNo ratings yet
- Lecture Euler EquationDocument33 pagesLecture Euler EquationYash RajNo ratings yet
- Reprocessing Guide: Shaver Handpiece TrayDocument198 pagesReprocessing Guide: Shaver Handpiece TrayAnne Stephany ZambranoNo ratings yet
- Mechanism of Heat TransferDocument31 pagesMechanism of Heat Transferedna padreNo ratings yet