You might also like
- Waiters' Training ManualDocument25 pagesWaiters' Training ManualKoustav Ghosh90% (51)
- Management of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryDocument4 pagesManagement of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryLatifa Hanif ZuhriNo ratings yet
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Essential Tissue Healing of the Face and NeckFrom EverandEssential Tissue Healing of the Face and NeckRating: 5 out of 5 stars5/5 (2)
- NASA: 181330main Jun29colorDocument8 pagesNASA: 181330main Jun29colorNASAdocumentsNo ratings yet
- Polishing Amalgam RestorationsDocument39 pagesPolishing Amalgam RestorationsMuad AbulohomNo ratings yet
- An Improved Glass Ionomer Restorative System for Class I and II RestorationsDocument7 pagesAn Improved Glass Ionomer Restorative System for Class I and II RestorationsKranti PrajapatiNo ratings yet
- 10867-0 Neoss Anatomical Healing Abutment Manual Hi Res 2009-05-19Document4 pages10867-0 Neoss Anatomical Healing Abutment Manual Hi Res 2009-05-19Nate TaylorNo ratings yet
- Space RegainerDocument7 pagesSpace RegainerdelfNo ratings yet
- Insertion of Complete DentureDocument6 pagesInsertion of Complete DentureMaulida Dara HarjantiNo ratings yet
- Comparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudyDocument132 pagesComparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudySkAliHassanNo ratings yet
- No Prep Veneers: A Guide to the ProcedureDocument20 pagesNo Prep Veneers: A Guide to the ProcedureratrikaruniaNo ratings yet
- Presentation1 PdiDocument51 pagesPresentation1 PdiAisha samreenNo ratings yet
- Pre-Prosthetic Treatment and Tooth PreparationDocument45 pagesPre-Prosthetic Treatment and Tooth PreparationJody JodzNo ratings yet
- Fixed Partial Denture GuideDocument25 pagesFixed Partial Denture GuideKyrkNo ratings yet
- Chu's Aesthetic Gauge BrochureDocument2 pagesChu's Aesthetic Gauge BrochureHugoRoCkstarNo ratings yet
- Space Regainers in Pediatric DentistryDocument6 pagesSpace Regainers in Pediatric DentistryFayiz SäbNo ratings yet
- Modified Bluegrass Appliance PDFDocument4 pagesModified Bluegrass Appliance PDFRenieKumalaNo ratings yet
- Prefabricated Fiber PostDocument10 pagesPrefabricated Fiber PostRanuch TakNo ratings yet
- Occlusal Considerations in ImplantDocument11 pagesOcclusal Considerations in ImplantRolzilah RohaniNo ratings yet
- FINAL SplintingDocument46 pagesFINAL SplintingDilmohit SinghNo ratings yet
- Periodontal Surgery Consent FormDocument2 pagesPeriodontal Surgery Consent FormJitender ReddyNo ratings yet
- Section - 026 - Immediate DenturesDocument12 pagesSection - 026 - Immediate DenturesMuli Maroshi100% (1)
- Acc Pain FauziDocument8 pagesAcc Pain FauziMuchlis Fauzi ENo ratings yet
- New Microsoft Office Word DocumentDocument3 pagesNew Microsoft Office Word DocumentAtulsanapNo ratings yet
- Provisional Splinting 2013Document87 pagesProvisional Splinting 2013felicedaNo ratings yet
- Precision AttachmentsDocument2 pagesPrecision AttachmentsShree PrabhaNo ratings yet
- Frame Denture - Metal Frame BenefitsDocument8 pagesFrame Denture - Metal Frame BenefitsJennieNo ratings yet
- Journal of Prosthetic DentistryDocument7 pagesJournal of Prosthetic DentistryAmar BhochhibhoyaNo ratings yet
- Trauma From OcclusionDocument3 pagesTrauma From OcclusionSuganya MurugaiahNo ratings yet
- Cieszynski' Rule of IsometryDocument5 pagesCieszynski' Rule of Isometrynishant_tewari_1No ratings yet
- Implant Thread Designs: An Overview: July 2017Document10 pagesImplant Thread Designs: An Overview: July 2017Seno FauziNo ratings yet
- Tips On Access Cavity Preparation.: How To' TechniqueDocument4 pagesTips On Access Cavity Preparation.: How To' TechniqueGoran TosicNo ratings yet
- Iti ImplantDocument8 pagesIti ImplantMuaiyed Buzayan AkremyNo ratings yet
- Functional OcclusionDocument8 pagesFunctional OcclusionNoor SolikhahNo ratings yet
- Prosthodontic DiagnosisDocument15 pagesProsthodontic DiagnosisYashpreetsingh Bhatia100% (1)
- Basic Surgical Techniques For Endosseous Implant PlacementDocument101 pagesBasic Surgical Techniques For Endosseous Implant PlacementAnshuman Dwivedi100% (2)
- Single flap approach yields substantial CAL gain for deep intraosseous defectsDocument21 pagesSingle flap approach yields substantial CAL gain for deep intraosseous defectskarthikNo ratings yet
- Ally Treated Teeth As AbutmentsDocument6 pagesAlly Treated Teeth As AbutmentsLodi Al-SayedNo ratings yet
- Bds Tutorial Overdentures 1Document7 pagesBds Tutorial Overdentures 1ikeuchi_ogawaNo ratings yet
- DentureDocument80 pagesDentureDrShweta SainiNo ratings yet
- Dense Bone Island: Temuan Insidental Pada Radiograf PanoramikDocument4 pagesDense Bone Island: Temuan Insidental Pada Radiograf PanoramikFransiski HoNo ratings yet
- Selective GrindingDocument4 pagesSelective GrindingDentist HereNo ratings yet
- Implant Supported Overdentures GuideDocument32 pagesImplant Supported Overdentures GuideAkshayaa BalajiNo ratings yet
- Immediate DentureDocument52 pagesImmediate Denturedkdinesh020No ratings yet
- Fixed Partial Dentures 2Document153 pagesFixed Partial Dentures 2Mohsin Habib100% (1)
- Polyetheretherketone PEEK Dental Implants A Case FDocument8 pagesPolyetheretherketone PEEK Dental Implants A Case FPhoebe David100% (1)
- Effect of Splinting on Periodontal HealthDocument4 pagesEffect of Splinting on Periodontal HealthSweetz Viena ParamitaNo ratings yet
- Densah Bur Surgical Technique ManualDocument44 pagesDensah Bur Surgical Technique ManualLuis Felipe50% (2)
- Flexable Denture MaterialDocument28 pagesFlexable Denture MaterialSuvasish SuvasishNo ratings yet
- Bridge Indikasi & DesainDocument86 pagesBridge Indikasi & DesainFrieda Ayu PrihadiniNo ratings yet
- Complete Denture Insertion and Patient InstructionsDocument27 pagesComplete Denture Insertion and Patient InstructionsDrShweta SainiNo ratings yet
- Classification System For Full EdentulismDocument4 pagesClassification System For Full EdentulismmandakinimohanNo ratings yet
- Managing Root Fractures: Classification, Diagnosis and TreatmentDocument139 pagesManaging Root Fractures: Classification, Diagnosis and TreatmentHema lathaNo ratings yet
- Advances in Extraction TechniquesDocument13 pagesAdvances in Extraction TechniquesashajangamNo ratings yet
- Other Predisposing Factors of Dental CalculusDocument26 pagesOther Predisposing Factors of Dental CalculusKkumkum Swami100% (1)
- Food and Beverages Service: Learning MaterialsDocument24 pagesFood and Beverages Service: Learning MaterialsJoshua CondeNo ratings yet
- Kent Thiry IndictmentDocument10 pagesKent Thiry IndictmentMichael_Roberts2019No ratings yet
- Surveying 2 Practical 3Document15 pagesSurveying 2 Practical 3Huzefa AliNo ratings yet
- Business ModelsDocument10 pagesBusiness ModelsPiyushNo ratings yet
- Use VCDS with PC lacking InternetDocument1 pageUse VCDS with PC lacking Internetvali_nedeleaNo ratings yet
- Agility Logistics SolutionsDocument5 pagesAgility Logistics SolutionsWagner MontielNo ratings yet
- MgstreamDocument2 pagesMgstreamSaiful ManalaoNo ratings yet
- What Is ReligionDocument15 pagesWhat Is ReligionMary Glou Melo PadilloNo ratings yet
- Kim Hoff PAR 117 JDF 1115 Separation AgreementDocument9 pagesKim Hoff PAR 117 JDF 1115 Separation AgreementlegalparaeagleNo ratings yet
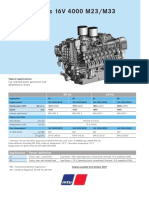
- Diesel Engines 16V 4000 M23/M33: 50 HZ 60 HZDocument2 pagesDiesel Engines 16V 4000 M23/M33: 50 HZ 60 HZAlberto100% (1)
- Harsheen Kaur BhasinDocument20 pagesHarsheen Kaur Bhasincalvin kleinNo ratings yet
- Form of SpesDocument2 pagesForm of SpesMark Dave SambranoNo ratings yet
- Kepler's ProblemDocument21 pagesKepler's ProblemGustavo MiasatoNo ratings yet
- Foreign AidDocument4 pagesForeign AidJesse JhangraNo ratings yet
- IN SUNNY SPAIN, 1882-85: "My Country, My Love, My People, I Leave You Now, You Disappear, I Lose Sight of You"Document4 pagesIN SUNNY SPAIN, 1882-85: "My Country, My Love, My People, I Leave You Now, You Disappear, I Lose Sight of You"Mary Claire ComalaNo ratings yet
- Water As A Weapon - Israel National NewsDocument11 pagesWater As A Weapon - Israel National NewsJorge Yitzhak Pachas0% (1)
- UITM Faculty of Business Entrepreneurship Rubric Social Media PortfolioDocument9 pagesUITM Faculty of Business Entrepreneurship Rubric Social Media PortfolioShamsyul AriffinNo ratings yet
- Quality Management in Apparel Industry PDFDocument9 pagesQuality Management in Apparel Industry PDFJyoti Rawal0% (1)
- Learning, Perception, Attitudes, Values, and Ethics: Fundamentals of Organizational Behavior 2eDocument21 pagesLearning, Perception, Attitudes, Values, and Ethics: Fundamentals of Organizational Behavior 2eJp AlvarezNo ratings yet
- Tax 1Document351 pagesTax 1AbbyNo ratings yet
- Diagrama RSAG7.820.7977Document14 pagesDiagrama RSAG7.820.7977Manuel Medina100% (4)
- Student (Mechanical Engineering), JECRC FOUNDATION, Jaipur (2) Assistant Professor, Department of Mechanical Engineering, JECRC FOUNDATION, JaipurDocument7 pagesStudent (Mechanical Engineering), JECRC FOUNDATION, Jaipur (2) Assistant Professor, Department of Mechanical Engineering, JECRC FOUNDATION, JaipurAkash yadavNo ratings yet
- Module IV StaffingDocument3 pagesModule IV Staffingyang_19250% (1)
- UNIT 2 Ielts Speaking Part 1 Questions Sample Answers IELTS FighterDocument15 pagesUNIT 2 Ielts Speaking Part 1 Questions Sample Answers IELTS FighterVi HoangNo ratings yet
- School RulesDocument2 pagesSchool RulesAI HUEYNo ratings yet
- The Oz DietDocument5 pagesThe Oz Dietkaren_wilkesNo ratings yet
- Emotion-WPS OfficeDocument2 pagesEmotion-WPS OfficemikaNo ratings yet
- Edited General English Question Paper Part 1Document12 pagesEdited General English Question Paper Part 1Utkarsh R MishraNo ratings yet