You might also like
- TASH CI HepatitisDocument47 pagesTASH CI HepatitisBeamlak Getachew WoldeselassieNo ratings yet
- Hepatitis Virus: Kurnia Dwi Artanti. Dept. of Epidemiology, Fac. of Public HealthDocument38 pagesHepatitis Virus: Kurnia Dwi Artanti. Dept. of Epidemiology, Fac. of Public Healthana fitrotulNo ratings yet
- (TM 2) Hepatitis B Dan CDocument59 pages(TM 2) Hepatitis B Dan CVivi OctaviaNo ratings yet
- Hepatitis B Dan CDocument59 pagesHepatitis B Dan CNafizah Nurul AidaNo ratings yet
- Seminar ProdiaDocument61 pagesSeminar ProdiaviraNo ratings yet
- Viral Hepatitis MBBS 2Document41 pagesViral Hepatitis MBBS 2Sohail ShahNo ratings yet
- Hepatitis Viruses Combination (Blood Borne Pathogens)Document51 pagesHepatitis Viruses Combination (Blood Borne Pathogens)Hosam GomaaNo ratings yet
- HBV GP PerspectiveDocument42 pagesHBV GP PerspectivePankaj IngleNo ratings yet
- L24 CLD-1Document60 pagesL24 CLD-1S sNo ratings yet
- Hepatitis Viruses OverviewDocument40 pagesHepatitis Viruses OverviewMeena CtNo ratings yet
- Viral Hepatitis-Dr. A.M IyagbaDocument62 pagesViral Hepatitis-Dr. A.M IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- 1hepatitis (HBV) 07Document47 pages1hepatitis (HBV) 07ganyetzNo ratings yet
- Hepatitis B - Virology: DNA Virus Class Hepadnaviridae TransmissionDocument6 pagesHepatitis B - Virology: DNA Virus Class Hepadnaviridae TransmissionDominic Delos SantosNo ratings yet
- Hepatitis Virus, Liver Cirrhosis and Hepatoma (HCCDocument61 pagesHepatitis Virus, Liver Cirrhosis and Hepatoma (HCCYun ZhaNo ratings yet
- Hepatitis B PDFDocument15 pagesHepatitis B PDFAvicenna_MSCNo ratings yet
- Viral Hepatitis (Virus Hepatitis)Document75 pagesViral Hepatitis (Virus Hepatitis)Ilmiah Bagus100% (1)
- VIRAL HEPATITIS CAUSES, SYMPTOMS AND DIAGNOSISDocument58 pagesVIRAL HEPATITIS CAUSES, SYMPTOMS AND DIAGNOSISMohammad Emad Al MadadhaNo ratings yet
- Hepatitis A, B and C: Causes, Symptoms and TestsDocument46 pagesHepatitis A, B and C: Causes, Symptoms and TestsChyzhi SylviaNo ratings yet
- Hepatitis Virus: Bagian Mikrobiologi FK UnissulaDocument36 pagesHepatitis Virus: Bagian Mikrobiologi FK UnissulaKarina Mega WNo ratings yet
- Therapeutic Strategies For Hepatitis B Virus Infection - Towards A CureDocument18 pagesTherapeutic Strategies For Hepatitis B Virus Infection - Towards A CureAdriana Villarreal FragaNo ratings yet
- Hepatitis A-E Viruses: An OverviewDocument49 pagesHepatitis A-E Viruses: An OverviewDeepak VermaNo ratings yet
- Presented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHDocument55 pagesPresented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHwira guna pratiwiNo ratings yet
- Hepatitis Viruses: VIRUS:Hepatitis A, B, CDocument25 pagesHepatitis Viruses: VIRUS:Hepatitis A, B, Carisita firmanNo ratings yet
- HepatitisDocument55 pagesHepatitisdebdeepbhattacharya411No ratings yet
- 1 HepatitisDocument62 pages1 HepatitisKamal AhmedNo ratings yet
- CCE090 Liver and Biliary TractDocument21 pagesCCE090 Liver and Biliary TractBharathi ManiyanNo ratings yet
- Infections of the Gastrointestinal TractDocument32 pagesInfections of the Gastrointestinal Tract180045No ratings yet
- Presented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHDocument55 pagesPresented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHKailash Nagar100% (1)
- Infectious Gastrointestinal Diseases: MicrobiologyDocument37 pagesInfectious Gastrointestinal Diseases: MicrobiologyRakesh KumarNo ratings yet
- Muhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarDocument54 pagesMuhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarPratiwi PurnamaNo ratings yet
- Hepatitis 1 (Viral Hepatitis)Document47 pagesHepatitis 1 (Viral Hepatitis)Louis TanNo ratings yet
- 3.0HEPATIT Lecture 5Document48 pages3.0HEPATIT Lecture 5Jiya MuhammadNo ratings yet
- HepatitisDocument24 pagesHepatitisAnn MariaNo ratings yet
- Type B hepatitis - the most common viral hepatitisDocument20 pagesType B hepatitis - the most common viral hepatitisBhupesh ChandNo ratings yet
- Hepatitis 4th - 2008 2009Document77 pagesHepatitis 4th - 2008 2009api-3827876No ratings yet
- Viral HepatitisDocument51 pagesViral HepatitisIlmiah BagusNo ratings yet
- Hepatitis Types and CausesDocument44 pagesHepatitis Types and CausesJosé Luis García GarcíaNo ratings yet
- Hepatitis B Dan C - PresentasiDocument31 pagesHepatitis B Dan C - PresentasiRatu anisa Fadila balgisNo ratings yet
- Hepatitis A-EDocument34 pagesHepatitis A-EVer Garcera TalosigNo ratings yet
- Hepatitis A GDocument23 pagesHepatitis A Gapi-3712326No ratings yet
- Hepatitis B Dalam KehamilanDocument15 pagesHepatitis B Dalam KehamilanjenniNo ratings yet
- Hepato-Billiary Diseases: Tutor: DR SocdaalDocument32 pagesHepato-Billiary Diseases: Tutor: DR SocdaalOmar mohamedNo ratings yet
- Hepatitis A-E Viruses: An OverviewDocument48 pagesHepatitis A-E Viruses: An OverviewPrajakta TawdeNo ratings yet
- Viral Hepatitis: DR - Abiy F. Nov 2019 Arsi UniversityDocument67 pagesViral Hepatitis: DR - Abiy F. Nov 2019 Arsi UniversityWakjira NigusuNo ratings yet
- Hepatitis B: Steve HartDocument36 pagesHepatitis B: Steve HartangelinaNo ratings yet
- Dr. G. Thiruvenkadam Post Graduate Dept of Pediatric & Preventive DentistryDocument31 pagesDr. G. Thiruvenkadam Post Graduate Dept of Pediatric & Preventive Dentistryதிருவேங்கடம் கோபாலன்No ratings yet
- Hepatitis BDocument25 pagesHepatitis BJevon AndraNo ratings yet
- Viral Hepatitis Clinical CorrelationDocument59 pagesViral Hepatitis Clinical Correlationdrhananfathy100% (3)
- Hepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetDocument48 pagesHepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetNurhidayahNo ratings yet
- Hepatitis B: Journal ReviewDocument41 pagesHepatitis B: Journal Reviewagita kartika sariNo ratings yet
- Chronic Viral HepatitisDocument66 pagesChronic Viral HepatitisSuresh KadliNo ratings yet
- 2 HBV & PidDocument43 pages2 HBV & PidHermela ShewangizawNo ratings yet
- Heaptobiliary Disease by Lecturio.Document106 pagesHeaptobiliary Disease by Lecturio.louisegantierNo ratings yet
- Swimming through Alphabet Soup: Viral hepatitis in 20 minsDocument17 pagesSwimming through Alphabet Soup: Viral hepatitis in 20 minsSaad KhanNo ratings yet
- Slide-Diagnosis Dan Interpretasi Hepatitis B KhronikDocument24 pagesSlide-Diagnosis Dan Interpretasi Hepatitis B KhronikSiti nur rohmahNo ratings yet
- Hepatitis and liver disease causes and treatmentsDocument42 pagesHepatitis and liver disease causes and treatmentsQusaiBadrNo ratings yet
- Challenges of Hepatitis B Infection in ChildrenDocument31 pagesChallenges of Hepatitis B Infection in ChildrenDr-Mohamed KadleNo ratings yet
- Viral Hepatitis: Nining Sri Wuryaningsih Bagian Patologi Klinik FK UNSDocument36 pagesViral Hepatitis: Nining Sri Wuryaningsih Bagian Patologi Klinik FK UNSdayanr02No ratings yet
- Hepatitis B Virus and Liver DiseaseFrom EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNo ratings yet
- Hepatitis C Virus-Host Interactions and Therapeutics: Current Insights and Future PerspectivesFrom EverandHepatitis C Virus-Host Interactions and Therapeutics: Current Insights and Future PerspectivesNo ratings yet
- Overview of HCV Epidemiology and Life CycleDocument15 pagesOverview of HCV Epidemiology and Life CycleEleni HagosNo ratings yet
- Viral Hepatitis Training Manual: Federal Ministry of Health National Hepatitis Control Program 2021Document22 pagesViral Hepatitis Training Manual: Federal Ministry of Health National Hepatitis Control Program 2021Eleni HagosNo ratings yet
- Viral Hepatitis Training Manual: Federal Ministry of Health National Hepatitis Control Program 2017Document44 pagesViral Hepatitis Training Manual: Federal Ministry of Health National Hepatitis Control Program 2017Eleni HagosNo ratings yet
- HBV VirologyDocument17 pagesHBV VirologyEleni HagosNo ratings yet
- Challenges of Achieving Viral Hepatitis Treatment Targets in EthiopiaDocument16 pagesChallenges of Achieving Viral Hepatitis Treatment Targets in EthiopiaEleni HagosNo ratings yet
- Challenges in VH Treatment: Fmoh 2021Document17 pagesChallenges in VH Treatment: Fmoh 2021Eleni HagosNo ratings yet
- HBV CasesDocument27 pagesHBV CasesEleni HagosNo ratings yet
- Programatic Management of Viral Hepatitis: Ministry of Health National HIV and Hepatitis Program 2021Document43 pagesProgramatic Management of Viral Hepatitis: Ministry of Health National HIV and Hepatitis Program 2021Eleni HagosNo ratings yet
- Viral Hepatitis Training Manual: Federal Ministry of Health National Hepatitis Control Program 2021Document11 pagesViral Hepatitis Training Manual: Federal Ministry of Health National Hepatitis Control Program 2021Eleni HagosNo ratings yet
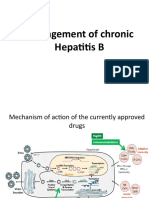
- Management of Chronic Hepatitis BDocument39 pagesManagement of Chronic Hepatitis BEleni HagosNo ratings yet
- HIV/HCV Co-InfectionDocument23 pagesHIV/HCV Co-InfectionEleni HagosNo ratings yet
- HIV/HCV Cases with DAA Treatment OptionsDocument23 pagesHIV/HCV Cases with DAA Treatment OptionsEleni HagosNo ratings yet
- HCV CasesDocument40 pagesHCV CasesEleni HagosNo ratings yet
- HBV-HIV Co-Infection CasesDocument11 pagesHBV-HIV Co-Infection CasesEleni HagosNo ratings yet
- Resistance in HCV: Andrew J. Muir, MD MHSDocument33 pagesResistance in HCV: Andrew J. Muir, MD MHSEleni HagosNo ratings yet
- Final National Malaria Guideline August 12 2022Document217 pagesFinal National Malaria Guideline August 12 2022Eleni Hagos67% (3)
- National Malaria Guideline 2022Document229 pagesNational Malaria Guideline 2022Eleni Hagos100% (4)
- HCV Treatment in Special Population: Difficult To Treat CasesDocument44 pagesHCV Treatment in Special Population: Difficult To Treat CasesEleni HagosNo ratings yet
- Malaria Case Management Training Manual For Health Professionals in Ethiopia Participants ManualDocument200 pagesMalaria Case Management Training Manual For Health Professionals in Ethiopia Participants ManualEleni HagosNo ratings yet
- Galloway 1989 Genetic Stratigraphic Sequence Basin Analysis IDocument18 pagesGalloway 1989 Genetic Stratigraphic Sequence Basin Analysis IMitreNo ratings yet
- Basavarajeshwari Group of Institutions: Self Balancing UnicycleDocument15 pagesBasavarajeshwari Group of Institutions: Self Balancing UnicycleJeerigi DeepikaNo ratings yet
- PhysicsDocument3 pagesPhysicsMohit TiwariNo ratings yet
- Treatment: Animated Text Onstage:: Topic: Learning Objective: WMS Packages Module Introduction Display 1Document8 pagesTreatment: Animated Text Onstage:: Topic: Learning Objective: WMS Packages Module Introduction Display 1hikikNo ratings yet
- German UnificationDocument40 pagesGerman UnificationJosephlangeloNo ratings yet
- IGO Operations Manual PDFDocument2,251 pagesIGO Operations Manual PDFMardi Wirengkoso100% (1)
- Nitrogen CycleDocument15 pagesNitrogen CycleKenji AlbellarNo ratings yet
- Global Detection - Electronic and Electromechanical Sensors Catalogue 2006.10 PDFDocument800 pagesGlobal Detection - Electronic and Electromechanical Sensors Catalogue 2006.10 PDFSarah RichardNo ratings yet
- Pharmaco-pornographic Politics and the New Gender EcologyDocument14 pagesPharmaco-pornographic Politics and the New Gender EcologyMgalo MgaloNo ratings yet
- A-PDF Watermark DEMO Purchase RemoveDocument4 pagesA-PDF Watermark DEMO Purchase RemoveGaurav JoshiNo ratings yet
- Personal Information SheetDocument4 pagesPersonal Information SheetLenny PangNo ratings yet
- LOGIK Fridge Freezer With Water Dispenser LSD55W18 ManualDocument20 pagesLOGIK Fridge Freezer With Water Dispenser LSD55W18 Manualfbunt2777No ratings yet
- Pharmaceutical and Software Development ProjectsDocument6 pagesPharmaceutical and Software Development ProjectsAlexandar123No ratings yet
- Orienteering Lesson PlanDocument34 pagesOrienteering Lesson PlanJuan Carlos Guillen BayonNo ratings yet
- KankanaP Phd2022Document243 pagesKankanaP Phd2022Mo NaNo ratings yet
- Kitne PakistanDocument2 pagesKitne PakistanAnkurNo ratings yet
- Congress Vienna QuestionsDocument5 pagesCongress Vienna QuestionsElliott CookNo ratings yet
- Dialogo Ingles 4 FinalDocument3 pagesDialogo Ingles 4 FinalJoae KsnsnsNo ratings yet
- 40 Inventive Principles Applied to Service OperationsDocument16 pages40 Inventive Principles Applied to Service Operationssina yadegariNo ratings yet
- Cardio Fitt Pin PostersDocument5 pagesCardio Fitt Pin Postersapi-385952225No ratings yet
- Herbivoría y Cristales de CaOxDocument33 pagesHerbivoría y Cristales de CaOxBrain LongwoodNo ratings yet
- 14-01 Lista de Laptops - DistribuidoresDocument29 pages14-01 Lista de Laptops - DistribuidoresInkil Orellana TorresNo ratings yet
- Carco h90vsDocument9 pagesCarco h90vsRoxana Elizabeth Valencia NavarrteNo ratings yet
- Dead Reckoning and Estimated PositionsDocument20 pagesDead Reckoning and Estimated Positionscarteani100% (1)
- Primary Maths Dissertation ExamplesDocument8 pagesPrimary Maths Dissertation ExamplesPaperWritersAlbuquerque100% (1)
- History All Pictures QuestionsDocument7 pagesHistory All Pictures QuestionsDivyansh RajoriaNo ratings yet
- PHL Ad 17 01 Operationalguidance 2017 Eng Ops Manual Adolescent Health Development ProgramDocument111 pagesPHL Ad 17 01 Operationalguidance 2017 Eng Ops Manual Adolescent Health Development ProgramJoanne G Haw GetidaNo ratings yet
- Aquilion ONE GENESIS Edition Transforming CTDocument40 pagesAquilion ONE GENESIS Edition Transforming CTSemeeeJuniorNo ratings yet
- Innovative Lp1 BlogDocument5 pagesInnovative Lp1 BlogArya ElizabethNo ratings yet
- Iag Narrative ReportDocument16 pagesIag Narrative ReportHoely SaintNo ratings yet