You might also like
- Tumours of The LarynxDocument90 pagesTumours of The LarynxDrravikumar BhandariNo ratings yet
- Untitled 1Document17 pagesUntitled 1Tiberiu CttNo ratings yet
- Laryngeal Cancer: Anatomy, Risk Factors, Staging and TreatmentDocument41 pagesLaryngeal Cancer: Anatomy, Risk Factors, Staging and TreatmentNidya PutriNo ratings yet
- Tumours of Larynx: Benign MalignantDocument43 pagesTumours of Larynx: Benign MalignantVandana RaviNo ratings yet
- Laryngeal CancerDocument19 pagesLaryngeal Cancerduong thi myNo ratings yet
- Calarynx 130814125710 Phpapp01Document33 pagesCalarynx 130814125710 Phpapp01Wael ShamyNo ratings yet
- Laryngel Cancer: It Is The Most Common Cancer of The Upper Aerodigestive TractDocument43 pagesLaryngel Cancer: It Is The Most Common Cancer of The Upper Aerodigestive Tract95 Parul KNo ratings yet
- Neck LumpDocument18 pagesNeck LumpJosh BurkeNo ratings yet
- Laryngeal Mass: John F. Mcguire, MD, MbaDocument33 pagesLaryngeal Mass: John F. Mcguire, MD, MbaIvan DarioNo ratings yet
- Benign and Malignant Diseases of the LarynxDocument28 pagesBenign and Malignant Diseases of the LarynxfaizNo ratings yet
- Nasopharyngeal Cancer: R1 Kittipong PoolketkitDocument41 pagesNasopharyngeal Cancer: R1 Kittipong PoolketkitLpsuedjNo ratings yet
- Salivary Gland Tumors: Marka Crittenden M.D. PH.DDocument54 pagesSalivary Gland Tumors: Marka Crittenden M.D. PH.DNeeti JainNo ratings yet
- Laryngeal CarcinomaDocument52 pagesLaryngeal CarcinomaEjay Jacob Ricamara67% (3)
- Canceroflarynx 131223002324 Phpapp02 PDFDocument15 pagesCanceroflarynx 131223002324 Phpapp02 PDFWael ShamyNo ratings yet
- Hypopharyngeal Cancer Treatment OptionsDocument32 pagesHypopharyngeal Cancer Treatment OptionsDurrikamil khattakNo ratings yet
- DR 180114164748Document43 pagesDR 180114164748Hasnain ToheedNo ratings yet
- Papillary and Follicular Thyroid Cancer: K. A. Ikram Hussain Final Year M.B.B.SDocument26 pagesPapillary and Follicular Thyroid Cancer: K. A. Ikram Hussain Final Year M.B.B.SAhsan JamilNo ratings yet
- Laryngeal Cancer Ali Asiry Last Copy 2Document102 pagesLaryngeal Cancer Ali Asiry Last Copy 2Atheer AbdulazizNo ratings yet
- Cancer OropharynxDocument108 pagesCancer OropharynxAshokNo ratings yet
- Head and Neck TumoursDocument50 pagesHead and Neck Tumoursene.dubemNo ratings yet
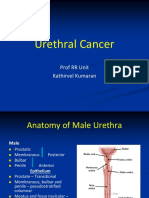
- Male Urethral Cancer Anatomy, Staging and TreatmentDocument24 pagesMale Urethral Cancer Anatomy, Staging and TreatmentKousik AmancharlaNo ratings yet
- Nasopharyngealcancer 170813182546Document56 pagesNasopharyngealcancer 170813182546kobexNo ratings yet
- Papillar y and Follicula R Thyroi D Cancer: K. A. Ikram Hussain Final Year M.B.B.SDocument26 pagesPapillar y and Follicula R Thyroi D Cancer: K. A. Ikram Hussain Final Year M.B.B.SAhsan JamilNo ratings yet
- Parapharyngeal Space TumorsDocument60 pagesParapharyngeal Space TumorsHossam ThabetNo ratings yet
- Management of Carcinoma Penis: DR Akhilesh Mishra Senior Resident Radiation Oncology Irch, AiimsDocument51 pagesManagement of Carcinoma Penis: DR Akhilesh Mishra Senior Resident Radiation Oncology Irch, AiimsWirawan Amirul BahriNo ratings yet
- Pharyngeal Tumours2Document46 pagesPharyngeal Tumours2miramirajalalNo ratings yet
- Lung Cancer: Understanding the PathophysiologyDocument70 pagesLung Cancer: Understanding the PathophysiologyLisa KurniaNo ratings yet
- Malignant Thyroid and Parathyroid DisordersDocument48 pagesMalignant Thyroid and Parathyroid DisordersPavan chowdaryNo ratings yet
- (PDF Copy) PSGSMMC Lecture - Reviewing Head and Neck Surgery 2021Document65 pages(PDF Copy) PSGSMMC Lecture - Reviewing Head and Neck Surgery 2021Patrick PengosroNo ratings yet
- M Sandamela Salivary Gland SandamelaDocument45 pagesM Sandamela Salivary Gland SandamelaRockson SamuelNo ratings yet
- Advanced Larynx CancerDocument23 pagesAdvanced Larynx Cancer李丞永No ratings yet
- Surgical Management of Malignant TumorsDocument129 pagesSurgical Management of Malignant TumorsAshish JainNo ratings yet
- Salivary Gland TumorDocument62 pagesSalivary Gland Tumordeepak kumarNo ratings yet
- Cervical Cancer Screening and TreatmentDocument104 pagesCervical Cancer Screening and TreatmentArie PratamaNo ratings yet
- Cups Neck by Dr. Musaib MushtaqDocument42 pagesCups Neck by Dr. Musaib MushtaqDr. Musaib MushtaqNo ratings yet
- MX Protocols Oropharyngeal Malignancy CompatDocument42 pagesMX Protocols Oropharyngeal Malignancy CompatBikram ChoudhuryNo ratings yet
- Tumors: of The Nose, Sinuses and NasopharynxDocument69 pagesTumors: of The Nose, Sinuses and Nasopharynxapi-19770621No ratings yet
- 3-3-08 KnudsonDocument27 pages3-3-08 KnudsonNurRahmaMusdalifaNo ratings yet
- Approach To STNDocument56 pagesApproach To STNAbhishek VaidyaNo ratings yet
- 12 Congenital Lesions of Larynx and Evaluation of StridorDocument77 pages12 Congenital Lesions of Larynx and Evaluation of StridorAbhishek ShahNo ratings yet
- LMR Ent - Throat: Diseases of Oral Cavity and Salivary GlandsDocument8 pagesLMR Ent - Throat: Diseases of Oral Cavity and Salivary GlandsYuku BabyNo ratings yet
- Testicular TumorsDocument6 pagesTesticular Tumorsyoussef.aziz2020No ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza HospitalDocument83 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza Hospitalpt.mahmoudNo ratings yet
- Thyroid CancerDocument38 pagesThyroid CancerNinikNo ratings yet
- Lymphatic Drainage of The Head & NeckDocument61 pagesLymphatic Drainage of The Head & NeckAishwarya S. Nair100% (1)
- Parapharyngeal Space Compatibility ModeDocument66 pagesParapharyngeal Space Compatibility ModeDrsiya MedfriendNo ratings yet
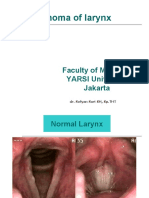
- Carcinoma of Larynx: Faculty of Medicine YARSI University JakartaDocument32 pagesCarcinoma of Larynx: Faculty of Medicine YARSI University JakartasantiNo ratings yet
- GCT in Males by Dr. Musaib MushtaqDocument44 pagesGCT in Males by Dr. Musaib MushtaqDr. Musaib MushtaqNo ratings yet
- Evaluation and Management of the Patient with a Neck MassDocument68 pagesEvaluation and Management of the Patient with a Neck MassFurqan MirzaNo ratings yet
- Thyroid Carcinoma - DR - NishanthDocument88 pagesThyroid Carcinoma - DR - Nishanth57- Kalanidhi mNo ratings yet
- Management of Ca LarynxDocument56 pagesManagement of Ca LarynxSatish Tripuraneni100% (1)
- Carcinoma of Larynx: Faculty of Medicine YARSI University JakartaDocument32 pagesCarcinoma of Larynx: Faculty of Medicine YARSI University JakartaAnnisa RobiyantiNo ratings yet
- PAROTID GLAND NEOPLASM IMAGINGDocument107 pagesPAROTID GLAND NEOPLASM IMAGINGigorNo ratings yet
- Laryngeal Cancer: Dr. Tan'Im Arief, SPTHT-KLDocument58 pagesLaryngeal Cancer: Dr. Tan'Im Arief, SPTHT-KLRani Dwi HapsariNo ratings yet
- Neck MassDocument40 pagesNeck Massdryojanasharma57100% (1)
- Laryngeal CancerDocument3 pagesLaryngeal Cancerneilclaudio0% (1)
- Gis 1 EnglishDocument85 pagesGis 1 Englishexand861No ratings yet
- Management of Throid CancerDocument65 pagesManagement of Throid Cancerد.صلاح مبروك خلافNo ratings yet
- Atlas of Parathyroid Imaging and PathologyFrom EverandAtlas of Parathyroid Imaging and PathologyAlexander L. ShifrinNo ratings yet
- 14 Benign Lesions of LarynxDocument80 pages14 Benign Lesions of LarynxAbhishek ShahNo ratings yet
- Inflammatory Disorders of the Larynx: Causes, Symptoms and TreatmentDocument83 pagesInflammatory Disorders of the Larynx: Causes, Symptoms and TreatmentAbhishek ShahNo ratings yet
- 12 Congenital Lesions of Larynx and Evaluation of StridorDocument77 pages12 Congenital Lesions of Larynx and Evaluation of StridorAbhishek ShahNo ratings yet
- Nasopharyngeal Angiofibroma Treatment OptionsDocument51 pagesNasopharyngeal Angiofibroma Treatment OptionsAbhishek ShahNo ratings yet
- 7 Neck Space InfectionsDocument99 pages7 Neck Space InfectionsAbhishek ShahNo ratings yet
- "First Time in History" - Cancer Vanishes For Every Patient in Drug TrialDocument3 pages"First Time in History" - Cancer Vanishes For Every Patient in Drug TrialDIPIN JAINNo ratings yet
- Giant Cell Tumor of The Phalanx of Finger: Case Reports: BackgroundDocument10 pagesGiant Cell Tumor of The Phalanx of Finger: Case Reports: BackgroundMoeez AkramNo ratings yet
- Agenda: The Plymouth Laryngectomy ClubDocument5 pagesAgenda: The Plymouth Laryngectomy ClubThe Plymouth Laryngectomy ClubNo ratings yet
- Session11-Premalignant Lesions of The Cervix, CX CADocument68 pagesSession11-Premalignant Lesions of The Cervix, CX CACHALIE MEQU100% (2)
- Guardant360 A0771104 v1 FinalDocument6 pagesGuardant360 A0771104 v1 FinaltraveltreatsteluguNo ratings yet
- Siddhesh PawarDocument1 pageSiddhesh PawarSiddhesh PawarNo ratings yet
- preliminary program simposium hpylori punta cana 2024Document5 pagespreliminary program simposium hpylori punta cana 2024api-737224042No ratings yet
- Jurnal Esophageal CancerDocument12 pagesJurnal Esophageal Cancerazza khalidahNo ratings yet
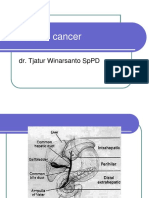
- Pancreatic Cancer: Dr. Tjatur Winarsanto SPPDDocument41 pagesPancreatic Cancer: Dr. Tjatur Winarsanto SPPDMayiz Renata LimerseNo ratings yet
- Chondroblastic Osteosarcoma in A Cat Case ReportDocument3 pagesChondroblastic Osteosarcoma in A Cat Case ReportMahdawwNo ratings yet
- Management of Gallbladder Polyps - An Optimal Strategy ProposedDocument4 pagesManagement of Gallbladder Polyps - An Optimal Strategy ProposedTANH NGUYENNo ratings yet
- The Timely Delivery of Radical Radiotherapy: Guidelines For The Management of Unscheduled Treatment InterruptionsDocument39 pagesThe Timely Delivery of Radical Radiotherapy: Guidelines For The Management of Unscheduled Treatment InterruptionsshreyaNo ratings yet
- An Introduction To Breast CancerDocument22 pagesAn Introduction To Breast Cancergiovanna2004No ratings yet
- Global Cancer Statistics 2018 - GLOBOCAN Estimates of Incidence and Mortality Worldwide For 36 Cancers in 185 CountriesDocument32 pagesGlobal Cancer Statistics 2018 - GLOBOCAN Estimates of Incidence and Mortality Worldwide For 36 Cancers in 185 CountriesGlauber MacielNo ratings yet
- (KULIAH) LimfomaDocument12 pages(KULIAH) Limfoma'Ilham Malda'No ratings yet
- Updates in The Eighth Edition of The Tumor-Node-Metastasis Staging Classification For Urologic CancersDocument10 pagesUpdates in The Eighth Edition of The Tumor-Node-Metastasis Staging Classification For Urologic CancersAbhishek PandeyNo ratings yet
- Imaging Head & Neck Inflammatory PseudotumorsDocument15 pagesImaging Head & Neck Inflammatory Pseudotumorskurnia hernolinggaNo ratings yet
- Melanoma-Skin-Cancer FinalDocument48 pagesMelanoma-Skin-Cancer FinalJeanessa Delantar QuilisadioNo ratings yet
- ĐÁP ÁN TIẾNG ANH CHUYÊN NGÀNH - Y DU KÍ MÙA 2Document7 pagesĐÁP ÁN TIẾNG ANH CHUYÊN NGÀNH - Y DU KÍ MÙA 2Lộc HuỳnhNo ratings yet
- CAR T Cell TherapyDocument16 pagesCAR T Cell TherapyRay SitepuNo ratings yet
- Pressurized Intraperitoneal Aerosol Chemotherapy With Oxaliplatin (PIPAC-OX) in Patients With Colorectal Peritoneal Metastases-A Systematic ReviewDocument17 pagesPressurized Intraperitoneal Aerosol Chemotherapy With Oxaliplatin (PIPAC-OX) in Patients With Colorectal Peritoneal Metastases-A Systematic Reviewcleanny espinozaNo ratings yet
- Bladder CancerDocument18 pagesBladder CancerjackbayNo ratings yet
- Guidelines For Management of Endometrial CarcinomaDocument41 pagesGuidelines For Management of Endometrial CarcinomaVeenaNo ratings yet
- Pasay City General Hospital Endoscopy Unit RequestDocument3 pagesPasay City General Hospital Endoscopy Unit RequestPeter Paul PascualNo ratings yet
- Basic Principles of Radiation OncologyDocument34 pagesBasic Principles of Radiation OncologyEstiani Ningsih100% (1)
- ANGIOSARCOMA A Rare Cause of Pleural MalignancyDocument3 pagesANGIOSARCOMA A Rare Cause of Pleural MalignancyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- KASUS 3 Early Staged Breast CancerDocument27 pagesKASUS 3 Early Staged Breast CancerWadhe Omara TobingNo ratings yet
- Ewing SarcomaDocument12 pagesEwing SarcomaVany MaksumNo ratings yet
- Review Test QuestionsDocument3 pagesReview Test QuestionsMarichu BajadoNo ratings yet
- Exam 4Document10 pagesExam 4pauchanmnlNo ratings yet