You might also like
- Grodno State Medical University: Assistant Lecturer of The Department of OphthalmologyDocument37 pagesGrodno State Medical University: Assistant Lecturer of The Department of Ophthalmologypriti089No ratings yet
- Grodno State Medical University: Assistant Lecturer of The Department of OphthalmologyDocument37 pagesGrodno State Medical University: Assistant Lecturer of The Department of OphthalmologyDenisse LizarragaNo ratings yet
- Diagnosis and Management CellulitisDocument26 pagesDiagnosis and Management Cellulitisdermato mikosisNo ratings yet
- Skin and Soft Tissue Infection InfoDocument4 pagesSkin and Soft Tissue Infection InfoPresura Andreea IulianaNo ratings yet
- Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, Updated Edition - Periocular Infections PDFDocument10 pagesMandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, Updated Edition - Periocular Infections PDFCarimaGhalieNo ratings yet
- Cutaneous Abscess Furuncles and CarbuclesDocument25 pagesCutaneous Abscess Furuncles and Carbuclesazmmatgowher_1219266No ratings yet
- Journal Reading: Update On The Management of Infectious KeratitisDocument35 pagesJournal Reading: Update On The Management of Infectious KeratitisninataniaaaNo ratings yet
- Corneal Bacterial UlcerDocument48 pagesCorneal Bacterial UlcerAkansha Rastogi100% (1)
- Infectious DermatosesDocument41 pagesInfectious DermatosesJuma SammyNo ratings yet
- ToxoDocument10 pagesToxoDaniyal Aziz KhanNo ratings yet
- Common Bacterial Skin InfectionsDocument6 pagesCommon Bacterial Skin InfectionsagusNo ratings yet
- 792 Viral Protozoal Corneal UlcerDocument33 pages792 Viral Protozoal Corneal UlcerMounika PapireddyNo ratings yet
- Periorbital CellulitisDocument2 pagesPeriorbital CellulitisNurliyana GhazaliNo ratings yet
- Conditions of The CorneaDocument38 pagesConditions of The Corneac/risaaq yuusuf ColoowNo ratings yet
- Morning Report, WHC, 12/2/2010Document20 pagesMorning Report, WHC, 12/2/2010Mohit MehtaniNo ratings yet
- Conjunctivitis and Other Ocular Lesions Opthalmology ClassDocument43 pagesConjunctivitis and Other Ocular Lesions Opthalmology ClassJaikrit SinghNo ratings yet
- Ojo RojoDocument7 pagesOjo Rojoapi-3696901No ratings yet
- Cellulitis: Clinical PracticeDocument9 pagesCellulitis: Clinical PracticeBobby S PromondoNo ratings yet
- Group 8 Parasitic CystsDocument47 pagesGroup 8 Parasitic CystsMariam Abd ElhadiNo ratings yet
- Corneal Ulcer: Prepared By: Renuka Shrestha Roll No: 29 PBBN 3rd Year SMTCDocument41 pagesCorneal Ulcer: Prepared By: Renuka Shrestha Roll No: 29 PBBN 3rd Year SMTCsushma shresthaNo ratings yet
- Mycotic Diseases and PeriodontiumDocument43 pagesMycotic Diseases and PeriodontiumAhmed Tawfig GamalNo ratings yet
- Corneal Ulcer Diagnosis and TreatmentDocument15 pagesCorneal Ulcer Diagnosis and TreatmentKumar jit MaityNo ratings yet
- OnlineMedEd Notes Dermatology 2021Document8 pagesOnlineMedEd Notes Dermatology 2021kirannhyd100% (1)
- Ophthalmology - Diseases of CorneaDocument18 pagesOphthalmology - Diseases of CorneajbtcmdtjjvNo ratings yet
- DR - Gaurav Shukla DR - Jyoti Batra DR - Uma SridharDocument101 pagesDR - Gaurav Shukla DR - Jyoti Batra DR - Uma SridharGaurav shuklaNo ratings yet
- Eye Emergency: DR Abdelmoniem SaeedDocument63 pagesEye Emergency: DR Abdelmoniem SaeedYousef Al-AmeenNo ratings yet
- Diseases of External EarDocument19 pagesDiseases of External EarMohamed Khaled TahaNo ratings yet
- Celulitis PDFDocument9 pagesCelulitis PDFGazade GarciaNo ratings yet
- Baby Kiran Aged 7 Years Brought To The Emergency Opd Accomp: ScenarioDocument22 pagesBaby Kiran Aged 7 Years Brought To The Emergency Opd Accomp: ScenariobhavanaNo ratings yet
- Incision & Drainage of Abscess Group 9 4bDocument5 pagesIncision & Drainage of Abscess Group 9 4bGUDISELA ramyaNo ratings yet
- Keratitis-Conjunctivitis Classification & TypesDocument81 pagesKeratitis-Conjunctivitis Classification & TypesAngnes Dera MustikaNo ratings yet
- Afecciones Anorrectales Benignas Absceso Perianal, Fístula Anal, Hemorroides, Fisuras y Seno PilonidalDocument7 pagesAfecciones Anorrectales Benignas Absceso Perianal, Fístula Anal, Hemorroides, Fisuras y Seno PilonidalJoshua MaciasNo ratings yet
- Tugas BacaDocument20 pagesTugas BacaAyu WulansariNo ratings yet
- Ocular Manifestations of HIV: A ReviewDocument33 pagesOcular Manifestations of HIV: A Reviewhenok birukNo ratings yet
- InfectionDocument3 pagesInfectionAndrew BonusNo ratings yet
- Oralmucocele AcasereportDocument5 pagesOralmucocele AcasereportxxxNo ratings yet
- SIGNS SYMPTOMS BACTERIAL CONJUNCTIVITISDocument3 pagesSIGNS SYMPTOMS BACTERIAL CONJUNCTIVITISPamela Sidharta100% (1)
- Practical 19asaDocument7 pagesPractical 19asaraulmoreira319No ratings yet
- (ANDREWS) Folliculitis, Furuncle, CarbuncleDocument8 pages(ANDREWS) Folliculitis, Furuncle, CarbunclempsoletaNo ratings yet
- What is a skin infection? Types, causes, symptoms and treatmentsDocument42 pagesWhat is a skin infection? Types, causes, symptoms and treatmentsKathleen Daban RagudoNo ratings yet
- Corneal Inflammation: Types, Causes and Treatments of KeratitisDocument32 pagesCorneal Inflammation: Types, Causes and Treatments of KeratitiscrushnaNo ratings yet
- 3.bacterial Infection-2Document146 pages3.bacterial Infection-2Biruk WorkuNo ratings yet
- Group 4: Trapago Trebucias Trinidad Umiten Vega Ventura Villalon YabresDocument86 pagesGroup 4: Trapago Trebucias Trinidad Umiten Vega Ventura Villalon YabresHunterDrimsumNo ratings yet
- Oral Manifestation in HIV PatientsDocument39 pagesOral Manifestation in HIV PatientsSarah Putri AbellysaNo ratings yet
- Infective Conditions of Hand and SkinDocument80 pagesInfective Conditions of Hand and SkinGracie KathyNo ratings yet
- P.S Very Nice!! May Pa-Picture Si Mayora!:D: FolliculitisDocument7 pagesP.S Very Nice!! May Pa-Picture Si Mayora!:D: FolliculitisBea SartoNo ratings yet
- Burns - Infection, Risk ForDocument4 pagesBurns - Infection, Risk Formakyofrancis20No ratings yet
- Book Review - CellulitisDocument3 pagesBook Review - CellulitisMary RiveroNo ratings yet
- Impetigo Diagnosis and TreatmentDocument4 pagesImpetigo Diagnosis and TreatmentCoral Srinivasa RamaluNo ratings yet
- December 2013 What Is Necrotizing Fasciitis? What Are Its Causes? How Will You Manage Such A Case?Document3 pagesDecember 2013 What Is Necrotizing Fasciitis? What Are Its Causes? How Will You Manage Such A Case?Vaibhav BharatNo ratings yet
- Skin and Soft Tissue Infection GuidelineDocument11 pagesSkin and Soft Tissue Infection GuidelineSylvinho46No ratings yet
- JEADV Clinical Practice - 2022 - Absil - Scabies and Therapeutic Resistance Current Knowledge and Future PerspectivesDocument8 pagesJEADV Clinical Practice - 2022 - Absil - Scabies and Therapeutic Resistance Current Knowledge and Future Perspectivestravel doctorNo ratings yet
- Surgery: Cervical LymphadenopathyDocument42 pagesSurgery: Cervical LymphadenopathyAgustinaNo ratings yet
- Treating and Managing UveitisDocument4 pagesTreating and Managing UveitisMoses Karanja Jr.No ratings yet
- Psoriasis: Posted: 02 Aug 2010 11:18 PM PDTDocument5 pagesPsoriasis: Posted: 02 Aug 2010 11:18 PM PDTScamb TrekNo ratings yet
- Corneal Stromal Inflammation Associated With Systemic InfectionsDocument16 pagesCorneal Stromal Inflammation Associated With Systemic InfectionsNabita AuliaNo ratings yet
- Acanthamoeba Keratitis: DR Saransh Jain 08/06/2015Document42 pagesAcanthamoeba Keratitis: DR Saransh Jain 08/06/2015Defayudina Dafilianty RosatariaNo ratings yet
- 079 Muhammad Khairul Nizam Bin Khir 7.1Document30 pages079 Muhammad Khairul Nizam Bin Khir 7.1Ilham RafisNo ratings yet
- DR Vishali's PaperDocument9 pagesDR Vishali's PaperpoojasharmachdNo ratings yet
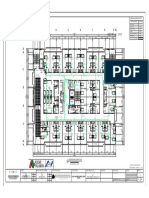
- ACE PALAWAN MGAS-SIXTH FLOOR-ModelDocument1 pageACE PALAWAN MGAS-SIXTH FLOOR-ModelBerlin Andrew SionNo ratings yet
- Super Top-Up Medicare Policy: United India Insurance Company LimitedDocument5 pagesSuper Top-Up Medicare Policy: United India Insurance Company LimitedGIJONo ratings yet
- NSMP FP For BHWsDocument30 pagesNSMP FP For BHWskristine ezpeletaNo ratings yet
- Cover LetterDocument1 pageCover Letterapi-354128955No ratings yet
- The Operating Room Charge Nurse: Coordinator and CommunicatorDocument5 pagesThe Operating Room Charge Nurse: Coordinator and Communicatordatabase badrusNo ratings yet
- Syringe Packs BrochureDocument2 pagesSyringe Packs BrochureIrinel BuscaNo ratings yet
- PHS 210 EpidemiologyDocument4 pagesPHS 210 EpidemiologySera GoldNo ratings yet
- RBM Business Plan (2009 - 2010)Document55 pagesRBM Business Plan (2009 - 2010)Amanze Donatus Uche100% (1)
- Sharon CVDocument3 pagesSharon CVDavis MitchelNo ratings yet
- National Guidelines On High Alert MedicationsDocument33 pagesNational Guidelines On High Alert Medicationsyunica simanjuntakNo ratings yet
- Pre-Medical NEET (UG), AIIMS Pre-Medical NEET (UG), AIIMS Pre-Medical NEET (UG), AIIMSDocument1 pagePre-Medical NEET (UG), AIIMS Pre-Medical NEET (UG), AIIMS Pre-Medical NEET (UG), AIIMSAditya PrasadNo ratings yet
- ANNEX A Masterlists of School Based Immunization 2019Document24 pagesANNEX A Masterlists of School Based Immunization 2019KRIZZIE JOY CAILINGNo ratings yet
- DRANK SauceDocument3 pagesDRANK SauceJery UnsfoldNo ratings yet
- IR - PERPUSTAAN UNIVERSITAS AIRLANGGADocument6 pagesIR - PERPUSTAAN UNIVERSITAS AIRLANGGAYuari AdeNo ratings yet
- Train The Trainer Manual PDFDocument146 pagesTrain The Trainer Manual PDFFootball Club AllianzNo ratings yet
- Part 1 - Cutlip and Center's Effective Public Relations. 11th Ed.Document127 pagesPart 1 - Cutlip and Center's Effective Public Relations. 11th Ed.Duyen Pham75% (4)
- NCMB317 RUBRICS Mental Status ExaminationDocument1 pageNCMB317 RUBRICS Mental Status Examinationkpbalay5921pamNo ratings yet
- Gastrointestinal Oncology - J. Abbruzzese, Et Al., (Oxford, 2004) WW PDFDocument938 pagesGastrointestinal Oncology - J. Abbruzzese, Et Al., (Oxford, 2004) WW PDFRaluca MărgulescuNo ratings yet
- Roles and Responsibilities of ASHADocument3 pagesRoles and Responsibilities of ASHAmohanpskohli8310No ratings yet
- Hotel LeadsDocument17 pagesHotel Leadssanakausar.5089No ratings yet
- Nature of Fraud and Its Effects in The Medical Insurance KenyaDocument12 pagesNature of Fraud and Its Effects in The Medical Insurance KenyaSaarah ConnieNo ratings yet
- How To Set Up A Pain ClinicDocument33 pagesHow To Set Up A Pain ClinicAmhae YunussNo ratings yet
- 090720-SANCARE SERVICE PROVIDER JuneDocument13 pages090720-SANCARE SERVICE PROVIDER JuneEdward AmanyireNo ratings yet
- Nurse Resume Mary Jane GorricetaDocument8 pagesNurse Resume Mary Jane GorricetaDick Morgan FerrerNo ratings yet
- Full Download Test Bank For Surgical Technology For The Surgical Technologist A Positive Care Approach 4th Edition PDF Full ChapterDocument36 pagesFull Download Test Bank For Surgical Technology For The Surgical Technologist A Positive Care Approach 4th Edition PDF Full Chapterbraidscanty8unib100% (18)
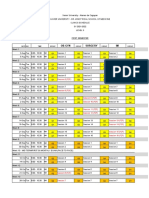
- Level 3 Clinics Schedule Clinics Groupings Group Leaders and PreceptorsDocument24 pagesLevel 3 Clinics Schedule Clinics Groupings Group Leaders and PreceptorsKIM LORIE YAP PASCUALNo ratings yet
- 8-File Utama Naskah-11-1-10-20200925Document7 pages8-File Utama Naskah-11-1-10-20200925Ade RatnasariNo ratings yet
- Ultrasound TherapyDocument3 pagesUltrasound Therapyليلى مسلمة100% (1)
- Medical SciencesDocument2 pagesMedical SciencesAŋdrés Melo100% (1)
- ToR of X-RayDocument3 pagesToR of X-RayAbdirahman Yusuf AliNo ratings yet