You might also like
- Basic Life Support (BLS) Provider HandbookFrom EverandBasic Life Support (BLS) Provider HandbookRating: 5 out of 5 stars5/5 (2)
- Newborn Priorities in First Days: RespirationDocument12 pagesNewborn Priorities in First Days: RespirationJoanna Bee Rose MagyawiNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Neonatal ResuscitationDocument15 pagesNeonatal ResuscitationAmruta GadeNo ratings yet
- How To Have an Easy and Safe Pregnancy and Bring Forth a Healthy Baby: A Pregnancy Book for First Time Moms for a Successful and Healthy Journey through Pregnancy, Childbirth and NewbornFrom EverandHow To Have an Easy and Safe Pregnancy and Bring Forth a Healthy Baby: A Pregnancy Book for First Time Moms for a Successful and Healthy Journey through Pregnancy, Childbirth and NewbornNo ratings yet
- Neonatal ResuscitationDocument16 pagesNeonatal ResuscitationPrecilla C. Stephen100% (3)
- Emergency Childbirth A Reference Guide for Students of the Medical Self-help Training Course, Lesson No. 11From EverandEmergency Childbirth A Reference Guide for Students of the Medical Self-help Training Course, Lesson No. 11No ratings yet
- Neonatal ResuscitationDocument15 pagesNeonatal Resuscitationpriyanka88% (8)
- Newborn Life Support: Resuscitation Council (UK)Document10 pagesNewborn Life Support: Resuscitation Council (UK)alvinatNo ratings yet
- Anatomy and Physiology of NeonatesDocument17 pagesAnatomy and Physiology of NeonatesYu ShiNo ratings yet
- Newborn ResuscitationDocument57 pagesNewborn ResuscitationmateenNo ratings yet
- Immediate Care of The NewbornDocument12 pagesImmediate Care of The NewbornLucilyn EbuengaNo ratings yet
- Essential Steps of Newborn ResuscitationDocument13 pagesEssential Steps of Newborn ResuscitationNikki SanchezNo ratings yet
- Newborn Resuscitation (Newborn CPR) BSN 12C: Madeline N. Gerzon, RN, MM Clinical Instructor Davao Doctors CollegeDocument59 pagesNewborn Resuscitation (Newborn CPR) BSN 12C: Madeline N. Gerzon, RN, MM Clinical Instructor Davao Doctors CollegemgerzonNo ratings yet
- High Risk NewbornDocument10 pagesHigh Risk NewbornEmmy Flor ValmoriaNo ratings yet
- NCM 107 Care of The Newborn Guide QuestionDocument5 pagesNCM 107 Care of The Newborn Guide QuestionMiguel LigasNo ratings yet
- Neonatal ResuscitationDocument28 pagesNeonatal ResuscitationDewi Rezeki ArbiNo ratings yet
- New Born ResuscitationDocument49 pagesNew Born ResuscitationdivyamuthyalaNo ratings yet
- Neonatal Resuscitation: Vineetha.T 1 Year MSC NursingDocument106 pagesNeonatal Resuscitation: Vineetha.T 1 Year MSC NursingVineetha ThachedathNo ratings yet
- Nursing Care For A High Risk NewbornDocument16 pagesNursing Care For A High Risk NewbornAj MacotoNo ratings yet
- Practical Aspects of Resuscitating Asphyxiated Newborn InfantsDocument5 pagesPractical Aspects of Resuscitating Asphyxiated Newborn InfantsFaiz ZidanNo ratings yet
- Module: Newborn Infant Suctioning: Learning Material 4Document8 pagesModule: Newborn Infant Suctioning: Learning Material 4Farah Jelimae BagniNo ratings yet
- Immediate Care of The NewbornDocument11 pagesImmediate Care of The NewbornHannahKarizaNo ratings yet
- Newborn ResuscitationDocument32 pagesNewborn ResuscitationVarna MohanNo ratings yet
- Suctioning The NewbornDocument7 pagesSuctioning The Newbornzeren.angeles.ihsNo ratings yet
- CARE OF THE NEWBORN - ncm107Document6 pagesCARE OF THE NEWBORN - ncm107Jasmin NatocNo ratings yet
- Essential Newborn Care GuideDocument120 pagesEssential Newborn Care Guidejuly3ciaNo ratings yet
- Neonatal Resuccitation: Practical &simplifiedDocument24 pagesNeonatal Resuccitation: Practical &simplifiedsali100% (1)
- Immediate Newborn Care and Breastfeeding InitiationDocument45 pagesImmediate Newborn Care and Breastfeeding InitiationRouquia ManzoorNo ratings yet
- Newborn Care StepsDocument58 pagesNewborn Care StepsMerlin AshlyNo ratings yet
- Golden First Minute 2Document9 pagesGolden First Minute 2meliaNo ratings yet
- II. AsfiksiaDocument41 pagesII. AsfiksiahazelelNo ratings yet
- Neonatal Resuscitation: BY DR Babatunde O.TDocument20 pagesNeonatal Resuscitation: BY DR Babatunde O.Tijojo elizabethNo ratings yet
- Newborn CareDocument51 pagesNewborn CareHurley ReefNo ratings yet
- Newborn Resuscitation EssentialsDocument34 pagesNewborn Resuscitation EssentialsVarna MohanNo ratings yet
- Resucition 2Document8 pagesResucition 2sudeepminz15No ratings yet
- Initiating and Maintaining RespirationsDocument2 pagesInitiating and Maintaining Respirationsitsjamyca najorraNo ratings yet
- CAREGIVING NC II - Week7Document12 pagesCAREGIVING NC II - Week7Lignerrac Anipal UtadNo ratings yet
- Infant RDSDocument3 pagesInfant RDSVenice Ramiro GamutanNo ratings yet
- Circulatory and Respiratory Adaptations in NeonatesDocument17 pagesCirculatory and Respiratory Adaptations in NeonatesGarry SoloanNo ratings yet
- Newborn CareDocument120 pagesNewborn CareMike CalipayanNo ratings yet
- Neonatal Resuscitation.Document18 pagesNeonatal Resuscitation.vrd2109No ratings yet
- Lesson (5) Neonatal ResuscitationDocument14 pagesLesson (5) Neonatal ResuscitationDrmirfat AlkashifNo ratings yet
- Resuscitation of The Newborn Anaesthesia TutorialDocument12 pagesResuscitation of The Newborn Anaesthesia TutorialJoana MoreiraNo ratings yet
- MCN FinalsDocument40 pagesMCN Finalsmolderoirish600No ratings yet
- Neonatal Resuscitation Techniques and EquipmentDocument54 pagesNeonatal Resuscitation Techniques and EquipmentdrkiranmNo ratings yet
- Keypoint For Lesson 1Document12 pagesKeypoint For Lesson 1Kishan ArrumugamNo ratings yet
- Foun Ations o Neonata R Esuscitation: What You Will LearnDocument12 pagesFoun Ations o Neonata R Esuscitation: What You Will LearnAndreaNo ratings yet
- Jurnal Astra ResusitasiDocument33 pagesJurnal Astra ResusitasiEta EtiiNo ratings yet
- Suctioning LectureDocument5 pagesSuctioning LectureAngelina Nicole G. TungolNo ratings yet
- Newborn Lecture HandoutDocument57 pagesNewborn Lecture HandoutChesca LayosaNo ratings yet
- New Born Care: Slide 0: Learning ObjectivesDocument10 pagesNew Born Care: Slide 0: Learning ObjectivesAmelia ChristmasNo ratings yet
- American Academy of PediatricsDocument320 pagesAmerican Academy of PediatricsJuan Sebasatián Arjona100% (2)
- ANZCOR Guideline 13.4 - Airway Management and Mask Ventilation of The NewbornDocument18 pagesANZCOR Guideline 13.4 - Airway Management and Mask Ventilation of The NewbornEssam HassanNo ratings yet
- New Born CareDocument17 pagesNew Born CareHarrison Tallod100% (1)
- Neonatal ResuscitationDocument34 pagesNeonatal ResuscitationAthul IgnatiusNo ratings yet
- Nursing Care of A Family C NewbornDocument18 pagesNursing Care of A Family C NewbornAudreySalvadorNo ratings yet
- Care of The Newborn PDFDocument5 pagesCare of The Newborn PDFzhai bambalan100% (2)
- NeonatalresuscitationDocument67 pagesNeonatalresuscitationfidaNo ratings yet
- 7 Protein Part 2 - StudentsDocument48 pages7 Protein Part 2 - StudentsWappy WepwepNo ratings yet
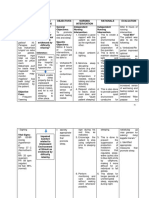
- Edited Readiness For Enhanced NutritionDocument4 pagesEdited Readiness For Enhanced NutritionWappy WepwepNo ratings yet
- Final Revision Impaired Comfort RT Unpleasant EnvironmentalDocument2 pagesFinal Revision Impaired Comfort RT Unpleasant EnvironmentalWappy WepwepNo ratings yet
- Test For Carbohydrates: Activity 6 Biochemistry LaboratoryDocument33 pagesTest For Carbohydrates: Activity 6 Biochemistry LaboratoryWappy Wepwep100% (2)
- Activity 7 Classifying of Sugars: Biochemistry LaboratoryDocument27 pagesActivity 7 Classifying of Sugars: Biochemistry LaboratoryWappy WepwepNo ratings yet
- Group Presentation: For Biochem Lab (Sg3)Document19 pagesGroup Presentation: For Biochem Lab (Sg3)Wappy WepwepNo ratings yet
- Score: Name: - Course: - Date: - Group No: - Activity 4 Diffusion and OsmosisDocument4 pagesScore: Name: - Course: - Date: - Group No: - Activity 4 Diffusion and OsmosisWappy WepwepNo ratings yet
- Observation Before Immersion After 15 Minutes of Immersion Starch Solution in The CellophaneDocument1 pageObservation Before Immersion After 15 Minutes of Immersion Starch Solution in The CellophaneWappy WepwepNo ratings yet
- Identification of Laboratory Apparatus and Its Uses: Presented by Group #4Document20 pagesIdentification of Laboratory Apparatus and Its Uses: Presented by Group #4Wappy WepwepNo ratings yet
- Score: Name: - Course: - Date: - Group No: - Activity 2 Organic ChemistryDocument4 pagesScore: Name: - Course: - Date: - Group No: - Activity 2 Organic ChemistryWappy Wepwep0% (1)
- Lesson 4 - The Business PlanDocument27 pagesLesson 4 - The Business PlanWappy Wepwep100% (1)
- Lesson 3 - Environment of Entrepreneurial VentureDocument25 pagesLesson 3 - Environment of Entrepreneurial VentureWappy WepwepNo ratings yet
- Lesson 2 - Entrepreneurial Character Traits, Skills, and COmpetenciesDocument40 pagesLesson 2 - Entrepreneurial Character Traits, Skills, and COmpetenciesWappy Wepwep100% (1)
- Score: Name: - Course: - Date: - Group No: - Activity 4 Diffusion and OsmosisDocument4 pagesScore: Name: - Course: - Date: - Group No: - Activity 4 Diffusion and OsmosisWappy WepwepNo ratings yet
- Social Stratification: Rich and Famous—or Rags and FamineDocument32 pagesSocial Stratification: Rich and Famous—or Rags and FamineWappy WepwepNo ratings yet
- DramaDocument6 pagesDramaWappy WepwepNo ratings yet
- Role of Starch Structure in Texture of Winter Squash (Cucurbita MDocument513 pagesRole of Starch Structure in Texture of Winter Squash (Cucurbita MWappy WepwepNo ratings yet
- Types of ResearchDocument37 pagesTypes of ResearchWappy WepwepNo ratings yet
- Nonfiction EssayDocument12 pagesNonfiction EssayWappy WepwepNo ratings yet
- Discussion Director: Introduction of The Author/WriterDocument2 pagesDiscussion Director: Introduction of The Author/WriterWappy WepwepNo ratings yet
- Nonfiction EssayDocument12 pagesNonfiction EssayWappy WepwepNo ratings yet
- Starch in Cucurbita MaximaDocument11 pagesStarch in Cucurbita MaximaWappy WepwepNo ratings yet
- Photoshop Cheat SheetDocument11 pagesPhotoshop Cheat SheetGiova RossiNo ratings yet
- Easy Eight's Battleground World War II Normandy NightmareDocument97 pagesEasy Eight's Battleground World War II Normandy NightmareAdolfo JoseNo ratings yet
- 1ST Quarter Exam Mapeh 8Document7 pages1ST Quarter Exam Mapeh 8John Rey Manolo BaylosisNo ratings yet
- Crescent Moon InstructionsDocument7 pagesCrescent Moon InstructionsSARANo ratings yet
- Env203Geo205 Map - ElementsDocument14 pagesEnv203Geo205 Map - ElementsFarhana SuptiNo ratings yet
- Iron Deficiency Anemia in ChildrenDocument27 pagesIron Deficiency Anemia in ChildrenAde Dinda WulandariNo ratings yet
- 2001 Bhuj EarthquakeDocument2 pages2001 Bhuj EarthquakeBhushanRajNo ratings yet
- The Columbian Exchange ReadingDocument3 pagesThe Columbian Exchange Readingapi-286657372No ratings yet
- Dynamic Programming Algorithm Explained in ECE 551 LectureDocument11 pagesDynamic Programming Algorithm Explained in ECE 551 Lectureadambose1990No ratings yet
- Trade BW Logistic ExtractionDocument54 pagesTrade BW Logistic Extractionlittlebros100% (1)
- Daniel Fast Recipes A Couple CooksDocument12 pagesDaniel Fast Recipes A Couple CooksmariamNo ratings yet
- Dh76 Auto HemaDocument271 pagesDh76 Auto HemaJoshua NarvaezNo ratings yet
- Quality Control and Assurance Processes for Coffee ProductionDocument5 pagesQuality Control and Assurance Processes for Coffee ProductionSharifah NuruljannahNo ratings yet
- CP306 Example 01 OKDocument5 pagesCP306 Example 01 OKManish MahadevwalaNo ratings yet
- Logix 5000 CIP Sync ConfigurationDocument180 pagesLogix 5000 CIP Sync Configurationاحتشام چوہدریNo ratings yet
- Ec6303 Signals and SystemsDocument2 pagesEc6303 Signals and SystemsSam PaulNo ratings yet
- MVC PaperDocument14 pagesMVC PaperManal MkNo ratings yet
- Solution:: Ex 3.3 Consider The Following Parallelograms. Find The Values of The Unknowns X, Y, ZDocument9 pagesSolution:: Ex 3.3 Consider The Following Parallelograms. Find The Values of The Unknowns X, Y, ZpadmaNo ratings yet
- Cape Physics U1 Ia BookletDocument10 pagesCape Physics U1 Ia Bookletedgeboy47100% (2)
- Shaw's play about a sculptor and his creationDocument8 pagesShaw's play about a sculptor and his creationEmanuel BurculetNo ratings yet
- VsamDocument24 pagesVsamRodrigoNo ratings yet
- BP Planning&Scheduling CaterpillarDocument35 pagesBP Planning&Scheduling CaterpillarOfelia Umpire Ruiz100% (4)
- Unit 4 FSQCDocument28 pagesUnit 4 FSQCvaralakshmi KNo ratings yet
- Panjab University, Chandigarh: (Theory Examinations) TIME OF EXAMINATION: 9.30 A.M. To 12.30 P.MDocument3 pagesPanjab University, Chandigarh: (Theory Examinations) TIME OF EXAMINATION: 9.30 A.M. To 12.30 P.MManav ChhabraNo ratings yet
- Master Gardener Home Vegetable Guide: Chapter 1 - Gardening BasicsDocument30 pagesMaster Gardener Home Vegetable Guide: Chapter 1 - Gardening BasicsAmr M. SaidNo ratings yet
- Summer Training Report Lean Process OptimisationDocument19 pagesSummer Training Report Lean Process OptimisationKrishna RaoNo ratings yet
- HypertensionDocument26 pagesHypertensionAbdalrhman Zaqqa100% (1)
- Vocabulary - Vocabulario de Salud y de Sintomas en InglesDocument4 pagesVocabulary - Vocabulario de Salud y de Sintomas en InglesCarlos MiguelNo ratings yet
- Commercial Kitchen Equipment CalculatorDocument16 pagesCommercial Kitchen Equipment CalculatorMohammad pharabiaNo ratings yet
- SAFETY GUIDELINES FOR FORMWORK AND CENTERINGDocument5 pagesSAFETY GUIDELINES FOR FORMWORK AND CENTERINGKrish VetriselvamNo ratings yet