You might also like
- ECA Report Request Form PDFDocument2 pagesECA Report Request Form PDFAfza Akbar100% (1)
- Kvaerner Hydro VALVESDocument24 pagesKvaerner Hydro VALVESEduardo CastilloNo ratings yet
- Problem Set 1 Man - EconDocument2 pagesProblem Set 1 Man - EconDW Waters100% (1)
- Cosmetic Otoplasty 2018 DBDocument11 pagesCosmetic Otoplasty 2018 DBcirugia plastica uisNo ratings yet
- Oshkosh M AtvDocument28 pagesOshkosh M AtvUsNdaomanu100% (1)
- RespiratoryDocument30 pagesRespiratorycainglesgaeaNo ratings yet
- Referensi3 AnatomiDocument10 pagesReferensi3 AnatominoviNo ratings yet
- 19 Via AereaDocument46 pages19 Via AereaCristian Mantilla medinaNo ratings yet
- Manejo Via AeraDocument6 pagesManejo Via AeraCarolin SantosNo ratings yet
- Internet Scientific PublicationsDocument12 pagesInternet Scientific PublicationsAnonymous h0DxuJTNo ratings yet
- Ent Exam 2023Document181 pagesEnt Exam 2023Syed NoorNo ratings yet
- Airway Management of A Vallecular Cyst Excision-A Nightmare To AnaesthetistsDocument3 pagesAirway Management of A Vallecular Cyst Excision-A Nightmare To AnaesthetistsIJAR JOURNALNo ratings yet
- Airway ManagmentDocument42 pagesAirway Managmentkader abdiNo ratings yet
- Respiratory SystemDocument54 pagesRespiratory SystemDominique MohanNo ratings yet
- Discovering Middle Ear Anatomy by Transcanal Endoscopic Ear Surgery: A Dissection ManualDocument8 pagesDiscovering Middle Ear Anatomy by Transcanal Endoscopic Ear Surgery: A Dissection ManualGuillermo Castro ContardoNo ratings yet
- Airway Assessment Predictors of Difficult AirwayDocument7 pagesAirway Assessment Predictors of Difficult AirwayChakib AmariNo ratings yet
- Airway Management, Ventilation, and Oxygen TherapyDocument56 pagesAirway Management, Ventilation, and Oxygen TherapybrentupdegraffNo ratings yet
- Anatomi Penginderaan: Ahmad Azwar Habibi Lab Anatomi FK UIN Syarif Hidayatullah JakartaDocument62 pagesAnatomi Penginderaan: Ahmad Azwar Habibi Lab Anatomi FK UIN Syarif Hidayatullah JakartaIin Widya Sari SiregarNo ratings yet
- Anatomi SSSDocument62 pagesAnatomi SSSIin Widya Sari SiregarNo ratings yet
- Rhinoscopyinthedog1 AnatomyandtechniquesDocument8 pagesRhinoscopyinthedog1 AnatomyandtechniquesZackiary YukiNo ratings yet
- Airway - Assessment - Predictors - of - Difficult - Airway HNDocument7 pagesAirway - Assessment - Predictors - of - Difficult - Airway HNfoolscribdNo ratings yet
- ENT Concept BookDocument177 pagesENT Concept BookPrincyNo ratings yet
- Laryngoscopy: OverviewDocument3 pagesLaryngoscopy: OverviewShazNo ratings yet
- SurgeryDocument606 pagesSurgeryDr. T. Balasubramanian100% (1)
- FERRIS in Basic Science Opthalmology Parte 1Document93 pagesFERRIS in Basic Science Opthalmology Parte 1Jhey RuilovaNo ratings yet
- RAJIV DHAWAN ENT FMG RR Watermark Final Corrected 09.11.23Document69 pagesRAJIV DHAWAN ENT FMG RR Watermark Final Corrected 09.11.23Wahib ZaidiNo ratings yet
- Anatomyof Paranasalsinuses Ent ScholarDocument13 pagesAnatomyof Paranasalsinuses Ent ScholarStancaMihaiAlexandruNo ratings yet
- 20.short Notes and Short Cases in ENT PDFDocument116 pages20.short Notes and Short Cases in ENT PDFpakistan100% (1)
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument28 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsFernaldy WiratamaNo ratings yet
- Tonsils-Are-Located-Between-Which-Two-Structures - HTML: D. Vestibular ApparatusDocument17 pagesTonsils-Are-Located-Between-Which-Two-Structures - HTML: D. Vestibular Apparatusmcycy miNo ratings yet
- ABCDE Assessment LecturioDocument12 pagesABCDE Assessment LecturioChristine Joy DeañoNo ratings yet
- Prediction Difficult AirwayDocument6 pagesPrediction Difficult AirwayParvathy R NairNo ratings yet
- By Tefera B (MSC.)Document55 pagesBy Tefera B (MSC.)Tofik MohammedNo ratings yet
- Mallampati Airway ClassificationDocument6 pagesMallampati Airway ClassificationAnthony Osemudiamen OseghaleNo ratings yet
- Vidian NeurectomyDocument54 pagesVidian NeurectomyDin PcNo ratings yet
- Breathing and Exchange of Gases by AA MamDocument10 pagesBreathing and Exchange of Gases by AA MamAks ChoudharyNo ratings yet
- MainDocument6 pagesMainDhio ArieyonaNo ratings yet
- ET Intubation and SuctioningDocument15 pagesET Intubation and SuctioningRenea Joy ArruejoNo ratings yet
- Surgical Option For Pediatric Bilateral Vocal Cord PalsyDocument9 pagesSurgical Option For Pediatric Bilateral Vocal Cord PalsyJeremy HermantoNo ratings yet
- Tonsil and Adenoid Anatomy: Edition: English Deutsch Español Français Português S PutriDocument5 pagesTonsil and Adenoid Anatomy: Edition: English Deutsch Español Français Português S PutriAdi HidayatNo ratings yet
- Paranasal Sinus Anatomy: What The Surgeon Needs To Know: June 2017Document36 pagesParanasal Sinus Anatomy: What The Surgeon Needs To Know: June 2017StancaMihaiAlexandruNo ratings yet
- Balingbing Histo LungsDocument5 pagesBalingbing Histo LungsJonas Zacarias BalingbingNo ratings yet
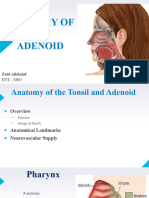
- Anatomy of The AdenoidDocument14 pagesAnatomy of The AdenoidZaid KhalafNo ratings yet
- Embryology and Anatomy of The Earoperative Techniques in OtolaryngologyDocument23 pagesEmbryology and Anatomy of The Earoperative Techniques in OtolaryngologyAtrik PristicaNo ratings yet
- Maged Shenawy PDFDocument403 pagesMaged Shenawy PDFObaid EllafyNo ratings yet
- Morghan Edisi 6 - 1Document34 pagesMorghan Edisi 6 - 1sarahNo ratings yet
- 22.07.2020 (Afternoon) FinalDocument79 pages22.07.2020 (Afternoon) Finalkrishan kumarNo ratings yet
- MGRUniv UGMar07Document32 pagesMGRUniv UGMar07Dr. T. BalasubramanianNo ratings yet
- An Unusual Cause of Stridor: Retropharyngeal Cold Abscess: Pediatric Surgery International April 2002Document4 pagesAn Unusual Cause of Stridor: Retropharyngeal Cold Abscess: Pediatric Surgery International April 2002akshayajainaNo ratings yet
- 07 - Ear TraumaDocument10 pages07 - Ear TraumaAhmad Rafi Satrio PrayogoNo ratings yet
- Larsens Human Embryology 468 495Document28 pagesLarsens Human Embryology 468 495Bintang PutraNo ratings yet
- Paranasal Sinus AnatomyDocument35 pagesParanasal Sinus AnatomyGeorge DaviesNo ratings yet
- Focused Ultrasound For AinwayDocument26 pagesFocused Ultrasound For AinwaywwtqfgtpNo ratings yet
- Anatomy RfeviewDocument2 pagesAnatomy Rfeviewgreen mateNo ratings yet
- Chapter 11 Gas Exchange in Humans 23-24Document127 pagesChapter 11 Gas Exchange in Humans 23-24Huraiza AsifNo ratings yet
- Tim Keperawatan Gawat DaruratDocument53 pagesTim Keperawatan Gawat Daruratjihan febriyantiNo ratings yet
- Enlarged Vestibular AqueductDocument86 pagesEnlarged Vestibular AqueductGhada WageihNo ratings yet
- Evaluationandmanagement Ofotalgia: Tiffany Peng Hwa,, Jason A. BrantDocument14 pagesEvaluationandmanagement Ofotalgia: Tiffany Peng Hwa,, Jason A. BrantLeo CortesNo ratings yet
- Wheezing Child...Document71 pagesWheezing Child...DawitNo ratings yet
- Anatomy, Physiology of ENT For Paramedics - Dr. Fuad RidhaDocument52 pagesAnatomy, Physiology of ENT For Paramedics - Dr. Fuad Ridhafuadredza100% (1)
- The Head and Neck Lectures: Anas Ibrahim YahayaDocument242 pagesThe Head and Neck Lectures: Anas Ibrahim YahayaBilkisu badamasiNo ratings yet
- Suprachoroidal Space InterventionsFrom EverandSuprachoroidal Space InterventionsShohista SaidkasimovaNo ratings yet
- Cleft Lip and Palate Management: A Comprehensive AtlasFrom EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNo ratings yet
- Hepatic AnesthesiaDocument43 pagesHepatic AnesthesiaBiserat GetnetNo ratings yet
- Anesthesia For Hepatic Resection and Laparascopic SurgeryDocument64 pagesAnesthesia For Hepatic Resection and Laparascopic SurgeryBiserat GetnetNo ratings yet
- Inhalational Anesthesia Mesi IIDocument64 pagesInhalational Anesthesia Mesi IIBiserat GetnetNo ratings yet
- Inhalational Anaesthesia Mesi IDocument84 pagesInhalational Anaesthesia Mesi IBiserat Getnet100% (1)
- ACID BASE BALANCE ModifiedDocument56 pagesACID BASE BALANCE ModifiedBiserat GetnetNo ratings yet
- Six Principles of Finance ManagementDocument5 pagesSix Principles of Finance ManagementAqib javed100% (1)
- E147478 BMW 5GT F07 NF FpoDocument9 pagesE147478 BMW 5GT F07 NF FpoInventyourselfNo ratings yet
- Digests PALEDocument11 pagesDigests PALEInter_vivosNo ratings yet
- Finishing and Polishing ProceduresDocument45 pagesFinishing and Polishing ProceduresDyuti SikdarNo ratings yet
- Bug Out Bag Essentials PDFDocument26 pagesBug Out Bag Essentials PDFJonathan Rea100% (2)
- Voluntary Winding Up and Removal of NamesDocument21 pagesVoluntary Winding Up and Removal of Namessreedevi sureshNo ratings yet
- Project CoordinatorDocument2 pagesProject Coordinatorapi-78653370No ratings yet
- LNG SummitDocument19 pagesLNG SummitRoozbeh PNo ratings yet
- Project Cost Management With 5D Bim: SciencedirectDocument8 pagesProject Cost Management With 5D Bim: Sciencedirectcrises7No ratings yet
- Slack Operations Management 6e Chapter1Document7 pagesSlack Operations Management 6e Chapter1dorislianNo ratings yet
- Grade Thresholds - June 2022: Cambridge IGCSE First Language English (Oral Endorsement) (0500)Document2 pagesGrade Thresholds - June 2022: Cambridge IGCSE First Language English (Oral Endorsement) (0500)Sufiyan ShahidNo ratings yet
- MIP291Document1 pageMIP291RogerioNo ratings yet
- CSRD March Board in BriefDocument2 pagesCSRD March Board in BriefaimhighsaNo ratings yet
- United States v. Scott Manning, Claimant-Appellant, 107 F.3d 5, 2d Cir. (1997)Document2 pagesUnited States v. Scott Manning, Claimant-Appellant, 107 F.3d 5, 2d Cir. (1997)Scribd Government DocsNo ratings yet
- Multiple Access Techniques LectureDocument23 pagesMultiple Access Techniques LecturefatimamanzoorNo ratings yet
- Motor Vechicle OrdinanceDocument127 pagesMotor Vechicle Ordinancemuhammad nazirNo ratings yet
- Land Laws Project ReportDocument19 pagesLand Laws Project ReportHarwinder Karra100% (1)
- Topic: A Study On Awareness and Accessing Behavior Of: DEMAT Account in Rajpipla CityDocument19 pagesTopic: A Study On Awareness and Accessing Behavior Of: DEMAT Account in Rajpipla CityBhavesh VasavaNo ratings yet
- HD 114 Jumbo Water Curtain NozzleDocument2 pagesHD 114 Jumbo Water Curtain Nozzlesun rockNo ratings yet
- GA5FF - tcm266 646875Document1 pageGA5FF - tcm266 646875peterpunk75No ratings yet
- 111 Ip Law 222Document81 pages111 Ip Law 222Leoni Francis LagramaNo ratings yet
- 6th Exam Time TableDocument21 pages6th Exam Time TableSunil ChoudhariNo ratings yet
- 16-00 Richard Tong Squirrel AIDocument25 pages16-00 Richard Tong Squirrel AIMohamed100% (1)
- Syllabus of Property LawDocument4 pagesSyllabus of Property LawpiyushNo ratings yet
- Eva I01-20230505Document11 pagesEva I01-20230505Digvijay KumarNo ratings yet
- SEA PrizrenDocument49 pagesSEA Prizrentom_hamm1008No ratings yet