You might also like
- ISMT 12 - Day 404 - Manefo - Minimally Invasive Posterior Cervical Foraminotomy and DiscectomyDocument20 pagesISMT 12 - Day 404 - Manefo - Minimally Invasive Posterior Cervical Foraminotomy and DiscectomyVito MasagusNo ratings yet
- Arthroscopy Assisted Tibial Plateau (Parafrase)Document22 pagesArthroscopy Assisted Tibial Plateau (Parafrase)vidiadityapamoriNo ratings yet
- Article. (Review) Laparoscopic Surgery For Rectal Cancer.2009Document6 pagesArticle. (Review) Laparoscopic Surgery For Rectal Cancer.2009Trí Cương NguyễnNo ratings yet
- Erector Spinae Plane Blocks For Traumatic Rib Fractures: A Prospective, Interventional Study - BenjaDocument1 pageErector Spinae Plane Blocks For Traumatic Rib Fractures: A Prospective, Interventional Study - BenjaFar HrNo ratings yet
- The Radiology Assistant - CT in TraumaDocument18 pagesThe Radiology Assistant - CT in Traumaابو عبد الرحمنNo ratings yet
- LWBK836 Ch98 p1021-1030Document10 pagesLWBK836 Ch98 p1021-1030metasoniko81No ratings yet
- Amputation and Rehabilitation 2010Document4 pagesAmputation and Rehabilitation 2010Amal KamalNo ratings yet
- ZJ 4852Document10 pagesZJ 4852Christopher BermeoNo ratings yet
- Abordagem Lateral ExtracavitáriaDocument9 pagesAbordagem Lateral ExtracavitáriaMarcelo MudoNo ratings yet
- Shoulder SurgeryDocument6 pagesShoulder Surgeryppica8111No ratings yet
- Modified Subvastus Approach With Improved Exposure.40Document3 pagesModified Subvastus Approach With Improved Exposure.40Bane StarcevicNo ratings yet
- Banc Zero W Ski 2014Document16 pagesBanc Zero W Ski 2014Vitória GuimarãesNo ratings yet
- Oosterlinck Et Al 2023 Minimally Invasive Coronary Surgery How Should It Be DefinedDocument6 pagesOosterlinck Et Al 2023 Minimally Invasive Coronary Surgery How Should It Be DefinedjafarkassimNo ratings yet
- Medi 96 E5936Document5 pagesMedi 96 E5936arm.solis32No ratings yet
- 1.principles of Oral SurgeryDocument13 pages1.principles of Oral SurgerydrpnnreddyNo ratings yet
- Below Knee AmputationDocument8 pagesBelow Knee AmputationJohan harjono100% (3)
- Lower Limb BlocksDocument5 pagesLower Limb BlocksParvathy R NairNo ratings yet
- Mapa Mental Profesional ColoridoDocument2 pagesMapa Mental Profesional Coloridoapi-634258689No ratings yet
- A Minimally Invasive Strategy For Breast Reconstruction: Latissimus Dorsi Muscle Flap Harvest by Single-Port EndosDocument4 pagesA Minimally Invasive Strategy For Breast Reconstruction: Latissimus Dorsi Muscle Flap Harvest by Single-Port EndosPutri Natasia KinskiNo ratings yet
- Cobb - Endoscopic Carpal Tunnel ReleaseDocument8 pagesCobb - Endoscopic Carpal Tunnel ReleaseJohnny WangNo ratings yet
- Anterior Anterolateral Posterior App Advantages DisadvantagesDocument8 pagesAnterior Anterolateral Posterior App Advantages Disadvantagesmuhammad bayu wicaksonoNo ratings yet
- AmputationDocument4 pagesAmputationFalah IsmailNo ratings yet
- Rib FractureDocument6 pagesRib FracturenasyilaputriNo ratings yet
- Completely Thoracoscopic Surgical StabilizationDocument9 pagesCompletely Thoracoscopic Surgical Stabilizationduke3443No ratings yet
- Small Incision Total Hip Replacement by The Lateral Approach Using Standard InstrumentsDocument5 pagesSmall Incision Total Hip Replacement by The Lateral Approach Using Standard InstrumentsApolinar González HernándezNo ratings yet
- Nursing-Surgery ConceptDocument19 pagesNursing-Surgery ConceptNoahdelNo ratings yet
- ISMT 12 - Day 403 - Vito - Cervical LaminoplastyDocument20 pagesISMT 12 - Day 403 - Vito - Cervical LaminoplastyVito MasagusNo ratings yet
- Emergency Laparoscopy A New Emerging Discipline For Treating Abdominal EmergenciesDocument13 pagesEmergency Laparoscopy A New Emerging Discipline For Treating Abdominal EmergenciesMarcus CezilloNo ratings yet
- PIIS0007091219306518Document3 pagesPIIS0007091219306518ZuraidaNo ratings yet
- Thoracic Incision For Open SurgeryDocument13 pagesThoracic Incision For Open SurgeryDavid IdowuNo ratings yet
- Minimally Invasive Treatment of Displaced Intra-Articular Calcaneal FracturesDocument14 pagesMinimally Invasive Treatment of Displaced Intra-Articular Calcaneal FracturesAnonymous kdBDppigENo ratings yet
- Transbuccal Approach For Management of Linear Ramus Fractures of Mandible: A Clinical TechniqueDocument6 pagesTransbuccal Approach For Management of Linear Ramus Fractures of Mandible: A Clinical TechniqueAB MISHRANo ratings yet
- Friel 2009Document17 pagesFriel 2009sidharthNo ratings yet
- Deigiudici2016 231022 130836Document7 pagesDeigiudici2016 231022 130836Cristian SanchezNo ratings yet
- Ultrasound-Guided Brachial Plexus BlockDocument7 pagesUltrasound-Guided Brachial Plexus BlockÇağdaş BaytarNo ratings yet
- Surgical Position Supino DecubbitusDocument4 pagesSurgical Position Supino DecubbitusMariana AmayaNo ratings yet
- Regional Anesthesia For Scapular Fracture Surgery: An Educational Review of Anatomy and TechniquesDocument6 pagesRegional Anesthesia For Scapular Fracture Surgery: An Educational Review of Anatomy and TechniquesSean SmythNo ratings yet
- Middle Fossa DiasDocument10 pagesMiddle Fossa DiasSebastianNo ratings yet
- Luxaciones Cadera 3Document11 pagesLuxaciones Cadera 3Sammy FarahNo ratings yet
- Surgical Management of Lumbar Spinal Stenosis: Rothman-Simeone and Herkowitz The Spine 7 EditionDocument41 pagesSurgical Management of Lumbar Spinal Stenosis: Rothman-Simeone and Herkowitz The Spine 7 Editionwira kusumaNo ratings yet
- Pre Peritoneal LaparoscópicaDocument16 pagesPre Peritoneal Laparoscópicamarquete72100% (1)
- Matrix RibDocument80 pagesMatrix RibTamara PricilaNo ratings yet
- Treatment of Orbital Lesions Using CyberKnife Stereotactic RadiosDocument1 pageTreatment of Orbital Lesions Using CyberKnife Stereotactic RadiosNesma OmdaNo ratings yet
- Acute Atelectasis Prevention & TreatmentDocument9 pagesAcute Atelectasis Prevention & TreatmentmetabolismeproteinNo ratings yet
- Flail ChestDocument8 pagesFlail ChestJaya PPDSNo ratings yet
- Retromandibular ApproachesDocument8 pagesRetromandibular ApproachesfsjNo ratings yet
- New Technique For Magnetic Compression Anastomosis.8Document10 pagesNew Technique For Magnetic Compression Anastomosis.8sjmc.surgeryresidentsNo ratings yet
- Thoracic Endoscopic Spine Surgery A ComprehensiveDocument11 pagesThoracic Endoscopic Spine Surgery A Comprehensivesanjay chhawraNo ratings yet
- Amputation and Rehabilitation 2013 Surgery OxfordDocument4 pagesAmputation and Rehabilitation 2013 Surgery OxfordSanjaya SenevirathneNo ratings yet
- Contralateral Approaches To Multiple Cerebral AneurysmsDocument4 pagesContralateral Approaches To Multiple Cerebral AneurysmsMorteza Mazloom Farsi BafNo ratings yet
- Retromandibular ApproachesDocument8 pagesRetromandibular ApproachesfsjNo ratings yet
- Inversion Therapy in Patients With Pure Single Level Lumbar Discogenic Disease: A Pilot Randomized TrialDocument8 pagesInversion Therapy in Patients With Pure Single Level Lumbar Discogenic Disease: A Pilot Randomized TrialPe T. ErNo ratings yet
- Role of Epidural AbdominalsurgeryDocument6 pagesRole of Epidural Abdominalsurgeryppica8111No ratings yet
- Case Report Stensrud2012Document13 pagesCase Report Stensrud2012marcus souzaNo ratings yet
- MV WeaknessDocument25 pagesMV WeaknessArmi ZakaNo ratings yet
- Above Elbow and Below Elbow AmputationDocument6 pagesAbove Elbow and Below Elbow AmputationJohan harjonoNo ratings yet
- Leak Rate Than Double-Stapled Technique After Minimally Invasive Total Mesorectal Excision For MRI-defined Low Rectal CancerDocument7 pagesLeak Rate Than Double-Stapled Technique After Minimally Invasive Total Mesorectal Excision For MRI-defined Low Rectal CancerRolando NavarroNo ratings yet
- SurgeryDocument6 pagesSurgeryEthan HuntNo ratings yet
- Contemporary Endoscopic Spine Surgery Volume 1: Cervical SpineFrom EverandContemporary Endoscopic Spine Surgery Volume 1: Cervical SpineNo ratings yet
- Ismt 12 - Day 414 - Bob - Mis TlifDocument12 pagesIsmt 12 - Day 414 - Bob - Mis TlifVito MasagusNo ratings yet
- Awake Glioma Surgery: Technical Evolution and NuancesDocument32 pagesAwake Glioma Surgery: Technical Evolution and NuancesVito MasagusNo ratings yet
- ISMT 12 - Day 396 - Manefo - Surgical Techniques For Peripheral Nerve RepairDocument23 pagesISMT 12 - Day 396 - Manefo - Surgical Techniques For Peripheral Nerve RepairVito MasagusNo ratings yet
- ISMT 12 - Day 400 - Brahma - Posterior Cervical Fusion Surgery - Occiput To C2Document16 pagesISMT 12 - Day 400 - Brahma - Posterior Cervical Fusion Surgery - Occiput To C2Vito MasagusNo ratings yet
- ISMT 12 - Day 403 - Vito - Cervical LaminoplastyDocument20 pagesISMT 12 - Day 403 - Vito - Cervical LaminoplastyVito MasagusNo ratings yet
- ISMT 12 - Day 402 - Rita - Posterior Cervical Laminectomy and Fusion Surgery C3-C7Document21 pagesISMT 12 - Day 402 - Rita - Posterior Cervical Laminectomy and Fusion Surgery C3-C7Vito MasagusNo ratings yet
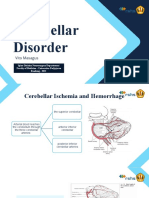
- ISMT12 - Day 457 - Vito - Cerebellar DisorderDocument17 pagesISMT12 - Day 457 - Vito - Cerebellar DisorderVito MasagusNo ratings yet
- ISMT 12 - Day 396 - Manefo - Harvesting Techniques of Cutaneous Nerves For GraftingDocument23 pagesISMT 12 - Day 396 - Manefo - Harvesting Techniques of Cutaneous Nerves For GraftingVito MasagusNo ratings yet
- ISMT 12 - Day 384 - Bob - Lumboperitneal ShuntingDocument11 pagesISMT 12 - Day 384 - Bob - Lumboperitneal ShuntingVito MasagusNo ratings yet
- ISMT 12 - Day 385 - Ravanno - Image Guidance in Minimally Invasive Spinal SurgeryDocument17 pagesISMT 12 - Day 385 - Ravanno - Image Guidance in Minimally Invasive Spinal SurgeryVito MasagusNo ratings yet
- ISMT 12 - Day 394 - Vito - Surgical Exposure of Peripheral Nerves of The Lower ExtremityDocument23 pagesISMT 12 - Day 394 - Vito - Surgical Exposure of Peripheral Nerves of The Lower ExtremityVito MasagusNo ratings yet
- ISMT 12 - Day 383 - Vito - Sacroiliac Joint Fusion Indications and TechniquesDocument17 pagesISMT 12 - Day 383 - Vito - Sacroiliac Joint Fusion Indications and TechniquesVito MasagusNo ratings yet
- ISMT 12 - Day 383 - Vito - Lumbopelvic Fixation TechniquesDocument18 pagesISMT 12 - Day 383 - Vito - Lumbopelvic Fixation TechniquesVito MasagusNo ratings yet
- Elective - Anterior Lumbar Fusion & Anterolateral Lumbar FusionDocument25 pagesElective - Anterior Lumbar Fusion & Anterolateral Lumbar FusionVito MasagusNo ratings yet
- Anterior or Posterior Cervical Fusion and Posterior Cervical Foraminotomy or DecompressionDocument26 pagesAnterior or Posterior Cervical Fusion and Posterior Cervical Foraminotomy or DecompressionVito MasagusNo ratings yet
- ISMT 12 - Day 340 - Vito - Somatosensory SystemsDocument20 pagesISMT 12 - Day 340 - Vito - Somatosensory SystemsVito MasagusNo ratings yet
- ISMT 12 - Day 519 - Vito - Surgery For Epidural and Subdural HematomasDocument24 pagesISMT 12 - Day 519 - Vito - Surgery For Epidural and Subdural HematomasVito MasagusNo ratings yet
- Journal Reading Coffee With CirrhosisDocument15 pagesJournal Reading Coffee With CirrhosisVito MasagusNo ratings yet
- How To Read Brain CT ScanDocument45 pagesHow To Read Brain CT ScanVito MasagusNo ratings yet
- History of CRCDocument26 pagesHistory of CRCFlaviu Ionuț FaurNo ratings yet
- Occupational Risk of Hepatitis BDocument3 pagesOccupational Risk of Hepatitis BshaannivasNo ratings yet
- All India Institute of Medical Sciences Nagpur Department of Obstetrics and GynecologyDocument19 pagesAll India Institute of Medical Sciences Nagpur Department of Obstetrics and GynecologySugan GavaskarNo ratings yet
- DentistryDocument16 pagesDentistryMeka Syahputra56% (9)
- Extraction Consent: Parkside Family Dental Informed Consent Tooth RemovalDocument14 pagesExtraction Consent: Parkside Family Dental Informed Consent Tooth Removalraymundo.ledfNo ratings yet
- Grammersense3 SB Anskey 2 PDFDocument40 pagesGrammersense3 SB Anskey 2 PDFjfgfdfNo ratings yet
- List of Medical Facilities in India: WWW - Gov.ukDocument81 pagesList of Medical Facilities in India: WWW - Gov.ukShah PratikNo ratings yet
- PrioritizationDocument20 pagesPrioritizationPascal St Peter Nwaorgu100% (1)
- CCR3 4 831 PDFDocument7 pagesCCR3 4 831 PDFArmareality ArmarealityNo ratings yet
- Carton Manufacturing Defects Line 1 Line 2 Line 3 Total DefectsDocument31 pagesCarton Manufacturing Defects Line 1 Line 2 Line 3 Total Defectspeter25munchenNo ratings yet
- Anesthesia in Day Care SurgeryDocument143 pagesAnesthesia in Day Care SurgeryGmkmcNo ratings yet
- Risk Management Report of Surgical InstrumentsDocument20 pagesRisk Management Report of Surgical InstrumentsAlejandro Landinez100% (2)
- Khalid EL-Jack CV Updated 2023Document3 pagesKhalid EL-Jack CV Updated 2023mathewsymssNo ratings yet
- Surgical Causes of Acute Abdominal Pain in Pregnancy: ReviewDocument9 pagesSurgical Causes of Acute Abdominal Pain in Pregnancy: ReviewMayada OsmanNo ratings yet
- JurnalDocument5 pagesJurnalJamila JuwitaNo ratings yet
- ANSYS Fluent - CFD Software PDFDocument3 pagesANSYS Fluent - CFD Software PDFSafi AhmedNo ratings yet
- Ojolhns 10 Issue II Dec 2016 ColorDocument66 pagesOjolhns 10 Issue II Dec 2016 ColorAnonymous ST1Ot2GAHxNo ratings yet
- Myofascial Release in Patients During The Early Postoperative Period After Revascularisation of Coronary ArteriesDocument13 pagesMyofascial Release in Patients During The Early Postoperative Period After Revascularisation of Coronary Arteriesestefy140399No ratings yet
- Fractional CO2Document11 pagesFractional CO2Dokter RudyNo ratings yet
- E023721 FullDocument9 pagesE023721 Fulljimmy xanzNo ratings yet
- Industry ReportDocument50 pagesIndustry ReportAbhay100% (1)
- Drug Prescribing Pattern in Surgical Wards of A TeDocument6 pagesDrug Prescribing Pattern in Surgical Wards of A TeNiranjan ChapagainNo ratings yet
- Pfannenstil Incision and Nerve EntrapmentDocument9 pagesPfannenstil Incision and Nerve EntrapmentBeni BolngNo ratings yet
- Pressure Ulcers and Wound CareDocument52 pagesPressure Ulcers and Wound CareKarina Mega WNo ratings yet
- Hemorrhoidectomy (Romanca, Rosalejos)Document48 pagesHemorrhoidectomy (Romanca, Rosalejos)Chloie Marie RosalejosNo ratings yet
- Nursing Care Plan and Diagnosis For MastectomyDocument4 pagesNursing Care Plan and Diagnosis For MastectomyAngie Mandeoya100% (2)
- Catalogo Champion 2020Document48 pagesCatalogo Champion 2020Ricardo PardoNo ratings yet
- Respiratory Tract Infection: What Causes Appendicitis?Document2 pagesRespiratory Tract Infection: What Causes Appendicitis?Novi AulNo ratings yet
- Katalog - Urologie - E (1) GCM TutorialDocument54 pagesKatalog - Urologie - E (1) GCM TutorialHayder HussienNo ratings yet
- Fundamentals of NursingDocument31 pagesFundamentals of NursingAngelica Soriano93% (14)