You might also like
- Adult Congenital Heart Disease Board ReviewDocument79 pagesAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnNo ratings yet
- Simple Office SpirometryDocument42 pagesSimple Office SpirometryRoberto Merza III100% (4)
- Left Ventricular Assist DevicesDocument14 pagesLeft Ventricular Assist DevicesLuis Alberto Caneo VergaraNo ratings yet
- Interventional Cardiology Certification Examination Blueprint - American Board of Internal MedicineDocument3 pagesInterventional Cardiology Certification Examination Blueprint - American Board of Internal MedicineabimorgNo ratings yet
- Aortic Stenosis AmendillaDocument31 pagesAortic Stenosis AmendillaVadim BursacovschiNo ratings yet
- Handbook of Interventional Cardiac Procedures for Junior Cardiologists: A Summary of Current Cardiology LiteratureFrom EverandHandbook of Interventional Cardiac Procedures for Junior Cardiologists: A Summary of Current Cardiology LiteratureNo ratings yet
- Upper Gastrointestinal BleedingDocument3 pagesUpper Gastrointestinal Bleedingplayaz_dan2100% (1)
- ElectrocardiogramDocument52 pagesElectrocardiogramTuong HoangManhNo ratings yet
- Cardiac Pacemakers NewDocument108 pagesCardiac Pacemakers NewAlif Fanharnita BrilianaNo ratings yet
- TCTMD Wire SelectionDocument59 pagesTCTMD Wire SelectionAmir MahmoudNo ratings yet
- ICU One Pager EVD V11Document1 pageICU One Pager EVD V11Mohamed Mahmoud100% (1)
- MVR CabgDocument57 pagesMVR CabgRoshani sharmaNo ratings yet
- Hemodynamics in The Cath Lab 2Document45 pagesHemodynamics in The Cath Lab 2usfcards100% (1)
- Valvular Heart Disease and Non Cardiac Surgery: Lakshmi P. YalavarthyDocument44 pagesValvular Heart Disease and Non Cardiac Surgery: Lakshmi P. YalavarthyLakshmi YalavarthyNo ratings yet
- Cardiac Catheterization and MonitoringDocument40 pagesCardiac Catheterization and MonitoringMarissa Asim100% (1)
- Chad Pressors HandoutDocument12 pagesChad Pressors HandoutquelspectacleNo ratings yet
- Aortic Stenosis:: Updates in Diagnosis & ManagementDocument48 pagesAortic Stenosis:: Updates in Diagnosis & ManagementCuca PcelaNo ratings yet
- Overview of - Balloon CathetersDocument55 pagesOverview of - Balloon CathetersGirishNo ratings yet
- CNED SDLP Cardiac Cath Lab Recovery 20 Feb 2011 Final PDFDocument11 pagesCNED SDLP Cardiac Cath Lab Recovery 20 Feb 2011 Final PDFPhyu_Hnin_Nain_1914100% (2)
- Percutaneous InterventionsDocument55 pagesPercutaneous InterventionsShannon Bellamy-FoggNo ratings yet
- Hemodynamic Drug InfusionsDocument45 pagesHemodynamic Drug InfusionsDawit MucheNo ratings yet
- MayoclinprocDocument12 pagesMayoclinprocpriyaNo ratings yet
- Valvular Heart Disease To TW FinalDocument13 pagesValvular Heart Disease To TW FinalMohammed ElSayedNo ratings yet
- Coronary Angiogram and Percutaneous Coronary InterventionDocument9 pagesCoronary Angiogram and Percutaneous Coronary Interventionellaine0024100% (2)
- Cardiac Interventional Cath Lab Tech v4. Study GuideDocument2 pagesCardiac Interventional Cath Lab Tech v4. Study GuideRoric Thomas100% (1)
- Prosth ValvesDocument74 pagesProsth ValvesRavi ZoreNo ratings yet
- Knobology and ImagingDocument30 pagesKnobology and ImagingLeo Ii S. RomagosNo ratings yet
- CCD Guidelines 2023Document123 pagesCCD Guidelines 2023Cuong Nguyen Vu TheNo ratings yet
- Invasive Devices On CXRDocument1 pageInvasive Devices On CXRLaurensia Erlina NataliaNo ratings yet
- Temporary Pacemakers-SICU's 101 PrimerDocument51 pagesTemporary Pacemakers-SICU's 101 Primerwaqas_xsNo ratings yet
- Fluid and Electrolyte Balance in ICUDocument46 pagesFluid and Electrolyte Balance in ICUtapas_kbNo ratings yet
- How-to Manual for Pacemaker and ICD Devices: Procedures and ProgrammingFrom EverandHow-to Manual for Pacemaker and ICD Devices: Procedures and ProgrammingNo ratings yet
- Echocardiographic Evaluation of Acute Aortic SyndromesDocument30 pagesEchocardiographic Evaluation of Acute Aortic SyndromesserubimNo ratings yet
- Endovascular InterventionsFrom EverandEndovascular InterventionsJose M. WileyNo ratings yet
- 5 Min - Myocardial Strain AnalysisDocument26 pages5 Min - Myocardial Strain AnalysisAsim Kumar Biswas100% (1)
- Mitral Valve RepairDocument109 pagesMitral Valve RepairheldhiNo ratings yet
- Mechanical Circulatory Support OverviewDocument34 pagesMechanical Circulatory Support OverviewJohn100% (1)
- Nursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationDocument4 pagesNursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationCharlene Jacobe Cornista100% (1)
- Aortic Root FinalDocument82 pagesAortic Root FinalMustafa KamalNo ratings yet
- Ventricular Assist DeviceDocument12 pagesVentricular Assist DevicesamadonyNo ratings yet
- Monitoring Hemodynamic Utk MahasiswaDocument49 pagesMonitoring Hemodynamic Utk MahasiswaPratami Rieuwpassa IINo ratings yet
- ECG InterpretationDocument82 pagesECG InterpretationIin Widya Sari Siregar100% (1)
- Hepatic Vein FlowDocument14 pagesHepatic Vein FlowJORGENo ratings yet
- Copy-Question PapersDocument87 pagesCopy-Question Paperspooja patilNo ratings yet
- 06 Clinical Pathology MCQs With Answers 1Document29 pages06 Clinical Pathology MCQs With Answers 1Habib Ullah100% (1)
- Basics of CathlabDocument39 pagesBasics of CathlabMemon RazakNo ratings yet
- Pacing Week PresentationsDocument54 pagesPacing Week PresentationsjoejenningsNo ratings yet
- Advanced Endovascular Therapy of Aortic DiseaseFrom EverandAdvanced Endovascular Therapy of Aortic DiseaseAlan B. LumsdenNo ratings yet
- Four Phases of ExerciseDocument2 pagesFour Phases of Exercisekb100% (1)
- ECMO and Right Ventricular FailureDocument9 pagesECMO and Right Ventricular FailureLuis Fernando Morales JuradoNo ratings yet
- Pulmonary SequestrationDocument15 pagesPulmonary SequestrationEmily EresumaNo ratings yet
- Nursing Care of The NewbornDocument72 pagesNursing Care of The NewbornCathreen Agatha FuleNo ratings yet
- Catheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Document42 pagesCatheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Omkar GaonkarNo ratings yet
- Non Cardiac OpDocument21 pagesNon Cardiac Opc4ri5No ratings yet
- AGT Applied Anatomy Notes1.1Document69 pagesAGT Applied Anatomy Notes1.1Akshay ChauhanNo ratings yet
- Mechanisms of Cardiac Arrhythmias From Automatici+Document24 pagesMechanisms of Cardiac Arrhythmias From Automatici+Malar MannanNo ratings yet
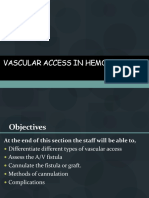
- Vascular Acess Number 1Document45 pagesVascular Acess Number 1Paulo GalangNo ratings yet
- Difficult Weaning From Cardiopulmonary Bypass Final Edit LiaDocument41 pagesDifficult Weaning From Cardiopulmonary Bypass Final Edit LiaYuri SadewoNo ratings yet
- Braunwald Lecture Series #2Document33 pagesBraunwald Lecture Series #2usfcards100% (2)
- Implementation of Low Delay Dual Chamber Pacemaker Using VerilogDocument4 pagesImplementation of Low Delay Dual Chamber Pacemaker Using VerilogMeghanand KumarNo ratings yet
- HUTTDocument25 pagesHUTTdrdj14100% (1)
- Dr. Dheeraj Sharma M.CH ResidentDocument94 pagesDr. Dheeraj Sharma M.CH ResidentVik SharNo ratings yet
- Harvesting The Radial ArteryDocument11 pagesHarvesting The Radial ArteryprofarmahNo ratings yet
- LVADDocument23 pagesLVADVashish RamrechaNo ratings yet
- Order ManagementDocument2 pagesOrder ManagementNeet Aipg newstipsNo ratings yet
- Scientific WorldDocument4 pagesScientific WorldNeet Aipg newstipsNo ratings yet
- Notice: National Board of ExaminationsDocument1 pageNotice: National Board of ExaminationsNeet Aipg newstipsNo ratings yet
- Journal Review 2Document1 pageJournal Review 2Neet Aipg newstipsNo ratings yet
- R1 R2 R3 R4: Learn CPR Strategy Stock Price Next Day PossibilityDocument4 pagesR1 R2 R3 R4: Learn CPR Strategy Stock Price Next Day PossibilityNeet Aipg newstipsNo ratings yet
- R1 R2 R3 R4: Learn CPR Strategy Stock Price Next Day PossibilityDocument4 pagesR1 R2 R3 R4: Learn CPR Strategy Stock Price Next Day PossibilityNeet Aipg newstipsNo ratings yet
- R1 R2 R3 R4: Learn CPR Strategy Stock Price Next Day PossibilityDocument4 pagesR1 R2 R3 R4: Learn CPR Strategy Stock Price Next Day PossibilityNeet Aipg newstipsNo ratings yet
- Treatment For Aplastic AnemiaDocument13 pagesTreatment For Aplastic Anemiagustianto hutama pNo ratings yet
- CPR Exam TheoryDocument10 pagesCPR Exam TheorysahirbuleNo ratings yet
- 1 of 1 - My Health SummaryDocument210 pages1 of 1 - My Health SummaryCandace DeihlNo ratings yet
- Alcoholic NeuropathyDocument11 pagesAlcoholic NeuropathyHuda HamoudaNo ratings yet
- Laryngitis and PericarditisDocument17 pagesLaryngitis and Pericarditis2B-4- TUNAC, Avvy Charlotte R.No ratings yet
- CHEST Journal - Single Article Antithrombotic Therapy For VTE Disease Antithrombotic Therapy For VTEDocument76 pagesCHEST Journal - Single Article Antithrombotic Therapy For VTE Disease Antithrombotic Therapy For VTEA. RaufNo ratings yet
- BreastfeedingDocument13 pagesBreastfeedingSintya AulinaNo ratings yet
- Learn To PredictDocument1 pageLearn To PredictKelley WalkerNo ratings yet
- Body Mechanics and Rom ExercisesDocument30 pagesBody Mechanics and Rom ExercisesWilma BeraldeNo ratings yet
- Case PresentationDocument138 pagesCase PresentationrinlopenaiNo ratings yet
- Nursing History: Biographic DataDocument2 pagesNursing History: Biographic DatayounggirldavidNo ratings yet
- Contoh Soal Skenario 4Document2 pagesContoh Soal Skenario 4NoNo ratings yet
- NCPDocument6 pagesNCPKrishna Faith P. DelaraNo ratings yet
- 10 Cancer Symptoms Women Shouldnt IgnoreDocument4 pages10 Cancer Symptoms Women Shouldnt IgnoreRavindra DubeyNo ratings yet
- Homeostasis QuestionsDocument9 pagesHomeostasis QuestionsJohn OsborneNo ratings yet
- Case ScenarioDocument3 pagesCase ScenarioKhyress Kyla BalalaNo ratings yet
- Evaluation of The Adult With Abdominal Pain - UpToDateDocument42 pagesEvaluation of The Adult With Abdominal Pain - UpToDateMario Lopez CastellanosNo ratings yet
- PART+B +Biopotential+AmplifiersDocument3 pagesPART+B +Biopotential+Amplifierselztly4694No ratings yet
- Manejo Radiológico de Las Masas de Partes Blandas de La Mano y MuñecaDocument28 pagesManejo Radiológico de Las Masas de Partes Blandas de La Mano y MuñecaJenniffer FNo ratings yet
- Bonus Task On Politics and GovernanceDocument3 pagesBonus Task On Politics and GovernanceVictorBaguilatNo ratings yet
- Comparison of The Short-Term Effectiveness of Short-Wave Diathermy Treatment in Patients With Carpal Tunnel Syndrome: A Randomized Controlled TrialDocument6 pagesComparison of The Short-Term Effectiveness of Short-Wave Diathermy Treatment in Patients With Carpal Tunnel Syndrome: A Randomized Controlled TrialChristine ViolaNo ratings yet
- Palmones Parasitology Lab TransesDocument19 pagesPalmones Parasitology Lab TransesJISOO KimNo ratings yet
- Textbook of NeuroimagingDocument403 pagesTextbook of NeuroimagingcelooshNo ratings yet
- Source E Learning NCM 121Document11 pagesSource E Learning NCM 121Nathaniel PulidoNo ratings yet
- Información: Estado Tipo de Participantes Rangos de EdadDocument11 pagesInformación: Estado Tipo de Participantes Rangos de EdadAlondraNo ratings yet
- Circulating Tumor Cells in Breast Cancer Metastatic DiseaseDocument177 pagesCirculating Tumor Cells in Breast Cancer Metastatic DiseaseAd AdrianaNo ratings yet