You might also like
- Chest & LungsDocument64 pagesChest & LungsStudenteeNo ratings yet
- Unit 06 Assessment of Thorax and LungDocument55 pagesUnit 06 Assessment of Thorax and Lunghuma100% (1)
- Lung Sounds: An Assessment of The Patient in Respiratory DistressDocument40 pagesLung Sounds: An Assessment of The Patient in Respiratory DistressJoseph Rodney de LeonNo ratings yet
- Lungs and ThoraxDocument9 pagesLungs and ThoraxMaria Mika Ella RetizaNo ratings yet
- Pemeriksaan Fisik Sistem Pernapasan: Equipment NeededDocument78 pagesPemeriksaan Fisik Sistem Pernapasan: Equipment Neededsri karinaNo ratings yet
- Examination of The Respiratory SystemDocument14 pagesExamination of The Respiratory SystemGopi JaladiNo ratings yet
- Respiratory Assessment 2Document24 pagesRespiratory Assessment 2Kendal BartonNo ratings yet
- Assessment of Respiratory System: Group 3Document33 pagesAssessment of Respiratory System: Group 3ChicieMonalisaNo ratings yet
- Nursing assessment techniquesDocument17 pagesNursing assessment techniquesJemmy KherisnaNo ratings yet
- Lung & Thorax Exams: Charlie Goldberg, M.D. Professor of Medicine, UCSD SOMDocument33 pagesLung & Thorax Exams: Charlie Goldberg, M.D. Professor of Medicine, UCSD SOMMuhammed BarznjiNo ratings yet
- Respiratory AssessmentDocument43 pagesRespiratory AssessmentLui Andrei AnilaNo ratings yet
- N1030 Theory Week 5 PPT - Student VersionDocument70 pagesN1030 Theory Week 5 PPT - Student Versiontksd7No ratings yet
- 1.2.4 Lung & RS Exam - SendDocument47 pages1.2.4 Lung & RS Exam - Senddanielndaa51No ratings yet
- CPAC-SON-HA-7-Thorax-1Document59 pagesCPAC-SON-HA-7-Thorax-1misshalieediiNo ratings yet
- Assessing The Thorax and The LungsDocument9 pagesAssessing The Thorax and The LungsChrizzia Del RosarioNo ratings yet
- Assessing The Thorax and The LungsDocument9 pagesAssessing The Thorax and The LungsChrizzia Del RosarioNo ratings yet
- Review NotesDocument9 pagesReview NotesKhaskie Geneva DumaguinNo ratings yet
- RSDocument12 pagesRSKamalchandra NaikNo ratings yet
- 8 Lung Auscultation Points and SoundsDocument11 pages8 Lung Auscultation Points and SoundsCHARIEMAE CA�AZARES100% (1)
- Pa Thorax LungsDocument88 pagesPa Thorax LungsLovelights ZamoraNo ratings yet
- Examination of Thorax and LungsDocument7 pagesExamination of Thorax and LungsJohanei Mae PeraltaNo ratings yet
- Anatomy & Physiology of Speech: - Speech Production Is Accomplished Via Three SystemsDocument30 pagesAnatomy & Physiology of Speech: - Speech Production Is Accomplished Via Three SystemsSwetha PasupuletiNo ratings yet
- Topic 1 - Pulmonary Anatomy, Physiology and Assessment (Hemo)Document39 pagesTopic 1 - Pulmonary Anatomy, Physiology and Assessment (Hemo)Ben JilhanoNo ratings yet
- Respiratory AssessmentDocument27 pagesRespiratory AssessmentAinaB ManaloNo ratings yet
- Respiratory SystemDocument23 pagesRespiratory SystemSaraNo ratings yet
- Thorax and The LungsDocument30 pagesThorax and The Lungschifunndo charles100% (1)
- 6 - Breath SoundsDocument31 pages6 - Breath SoundsggNo ratings yet
- Assessment of Respiratory SystemDocument34 pagesAssessment of Respiratory SystemKristal Jade Yanto Esquillo100% (1)
- Essential Parameters of Airway Evaluation Lecture 6Document27 pagesEssential Parameters of Airway Evaluation Lecture 69yqgmkvyzdNo ratings yet
- Examination of The Respiratory SystemDocument35 pagesExamination of The Respiratory SystemRashhmi Karthodi100% (1)
- Assessment of The Thorax and LungsDocument108 pagesAssessment of The Thorax and LungsJohn Martin Casihan100% (3)
- Lungs and Thorax Assessment - PPTX RAHEEM KHANDocument60 pagesLungs and Thorax Assessment - PPTX RAHEEM KHANRabia IsrafilNo ratings yet
- Assessment of The Thorax and Lungs 2014Document9 pagesAssessment of The Thorax and Lungs 2014alphabennydelta4468No ratings yet
- Assessment of the Respiratory SystemDocument20 pagesAssessment of the Respiratory SystemnadyaNo ratings yet
- F01 Thorax I (Chest and Lungs)Document113 pagesF01 Thorax I (Chest and Lungs)nonelNo ratings yet
- College of Nursing: 2 Semester (S.Y. 2021-2022)Document685 pagesCollege of Nursing: 2 Semester (S.Y. 2021-2022)Kristine Aranna ConcepcionNo ratings yet
- PEMERIKSAAN THORAX AND JANTUNGDocument59 pagesPEMERIKSAAN THORAX AND JANTUNGImada KhoironiNo ratings yet
- Respiratory AssessmentDocument79 pagesRespiratory AssessmentKarlo ReyesNo ratings yet
- Respiratorysystem 16Document35 pagesRespiratorysystem 16api-340406981No ratings yet
- Midterms SummaryDocument9 pagesMidterms SummarySAMSON, MAXZENE ANICKANo ratings yet
- The Anatomy and Physiology of The Respiratory SystemDocument26 pagesThe Anatomy and Physiology of The Respiratory SystemMonica Angelique SalayoNo ratings yet
- Assessment of The Chest and LungsDocument46 pagesAssessment of The Chest and LungsSumathi GopinathNo ratings yet
- Thorax and LungsDocument11 pagesThorax and LungsJoel SantosNo ratings yet
- Respiratory Exam GuideDocument18 pagesRespiratory Exam GuideIbi Yulia Setyani100% (1)
- Physical ExaminationDocument55 pagesPhysical Examinationdakshpanchal26369No ratings yet
- 5 - Respiratory AssessmentDocument61 pages5 - Respiratory AssessmentAbboud Ali100% (1)
- Physical Diagnoses: Respiratory SystemDocument72 pagesPhysical Diagnoses: Respiratory SystemAmanuel MaruNo ratings yet
- Pemeriksaan ThoraxDocument27 pagesPemeriksaan ThoraxSubchanPrasetyoNo ratings yet
- NCM 103 - Oxy RespiDocument21 pagesNCM 103 - Oxy RespiMaureen Gonzalo-FlorendoNo ratings yet
- Pemeriksaan ThoraxDocument27 pagesPemeriksaan ThoraxYaasinta ArlaesNo ratings yet
- Publication 2 21768 958Document41 pagesPublication 2 21768 958Safi MohammedNo ratings yet
- Respiratoryassessment 190701044607Document33 pagesRespiratoryassessment 190701044607wajidullah9551No ratings yet
- 1 - Internal Medicine UKIDocument128 pages1 - Internal Medicine UKILewishoppusNo ratings yet
- Kuliah Pengantar PF ParuDocument62 pagesKuliah Pengantar PF Parugagah152No ratings yet
- Lungs Assessment Associated With Cardiac DisorderDocument17 pagesLungs Assessment Associated With Cardiac DisorderdeepaNo ratings yet
- Resp Lecture FinalDocument37 pagesResp Lecture Finalapi-195799092No ratings yet
- 45 Mins or Less to Memorize, Pronounce and Understand Medical Terms. The Best and Most Effective Way to Build Your Medical Vocabulary Quickly!From Everand45 Mins or Less to Memorize, Pronounce and Understand Medical Terms. The Best and Most Effective Way to Build Your Medical Vocabulary Quickly!Rating: 2 out of 5 stars2/5 (2)
- Elimination-Homeostasis - StudentDocument16 pagesElimination-Homeostasis - StudentCruz YrNo ratings yet
- ContracturesDocument14 pagesContracturesCruz YrNo ratings yet
- Final Perioperative HomeostasisDocument33 pagesFinal Perioperative HomeostasisCruz YrNo ratings yet
- Family and Child Growth and Development - StudentDocument33 pagesFamily and Child Growth and Development - StudentCruz YrNo ratings yet
- Ethics in PediatricsDocument20 pagesEthics in PediatricsCruz YrNo ratings yet
- Diabetes Lecture Spring 2018-2Document101 pagesDiabetes Lecture Spring 2018-2Cruz YrNo ratings yet
- Disorders of GI Elimination Spring 19Document93 pagesDisorders of GI Elimination Spring 19Cruz YrNo ratings yet
- Disorders of Oxygenation Spring 17Document94 pagesDisorders of Oxygenation Spring 17Cruz YrNo ratings yet
- Concept Map Template Care PlanDocument1 pageConcept Map Template Care PlanCruz YrNo ratings yet
- Caring PPT Students EditDocument12 pagesCaring PPT Students EditCruz YrNo ratings yet
- Communicable Diseases PowerPoint - StudentDocument15 pagesCommunicable Diseases PowerPoint - StudentCruz YrNo ratings yet
- Cellular Regulation Student VersionDocument15 pagesCellular Regulation Student VersionCruz YrNo ratings yet
- Celluar and Neural Regulation StudentDocument52 pagesCelluar and Neural Regulation StudentCruz YrNo ratings yet
- Blood Gas Interpretation Review For PandemicDocument32 pagesBlood Gas Interpretation Review For PandemicJosilyn SalcedoNo ratings yet
- Biophysical ProfileDocument1 pageBiophysical ProfileCruz YrNo ratings yet
- 431 GMOandOrganicDocument36 pages431 GMOandOrganicCruz YrNo ratings yet
- Disassembly/Assembly: Primus® Family Breathing SystemDocument2 pagesDisassembly/Assembly: Primus® Family Breathing Systemheru pratiknoNo ratings yet
- Reading and Writing Skills Module 39999Document2 pagesReading and Writing Skills Module 39999Ericka Rivera SantosNo ratings yet
- NGNTestPacket 110322Document64 pagesNGNTestPacket 110322romeliza romeliza0% (1)
- Emergency First Aid GuideDocument21 pagesEmergency First Aid GuideJhelene AlyzzaNo ratings yet
- Co PilotDocument1 pageCo PilotdepdiaryNo ratings yet
- Respiratory System Lesson 2Document3 pagesRespiratory System Lesson 2Christopher EstevezNo ratings yet
- Laporan Pasien UGD PKM CIMSELDocument93 pagesLaporan Pasien UGD PKM CIMSELFianolly Putri RizkytianeNo ratings yet
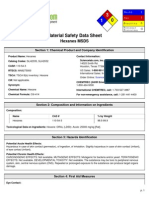
- MSDS HeksanaDocument6 pagesMSDS HeksanadiantikaNo ratings yet
- PICU Quiz: Critical ThinkingDocument4 pagesPICU Quiz: Critical ThinkingJehangir AllamNo ratings yet
- Chapter 1 The Human OrganismDocument12 pagesChapter 1 The Human OrganismJenny AnneNo ratings yet
- FITT 7 First Aid and Water Survival College of Criminal Justice (Loyola, Carl)Document4 pagesFITT 7 First Aid and Water Survival College of Criminal Justice (Loyola, Carl)Renzzo LoyolaNo ratings yet
- Reference: Piedad C. Pena (Et Al.) Biochemistry Laboratory Manual - 1 Ed. - Quezon City: C&E Publishing, Inc., 2015Document3 pagesReference: Piedad C. Pena (Et Al.) Biochemistry Laboratory Manual - 1 Ed. - Quezon City: C&E Publishing, Inc., 2015Kris Marie DelaCruz DomingoNo ratings yet
- K0K ( - 8 - 85 - 2 - PDFDocument162 pagesK0K ( - 8 - 85 - 2 - PDFCecilia LecuvaNo ratings yet
- Lalana Newborn ResuscitationDocument55 pagesLalana Newborn ResuscitationAthenaeum Scientific PublishersNo ratings yet
- Health 9 Learning Activity Sheet Quarter 3, Week 6-8Document4 pagesHealth 9 Learning Activity Sheet Quarter 3, Week 6-8fe delgadoNo ratings yet
- 2.2 First Aid - Basic First Aid and Resuscitation - Participant HandoutDocument3 pages2.2 First Aid - Basic First Aid and Resuscitation - Participant HandoutEva ChristinaNo ratings yet
- The Actor's Secret - Five Alexander Technique Tips For The ActorDocument3 pagesThe Actor's Secret - Five Alexander Technique Tips For The ActorLeland Vall80% (5)
- SDS 791471000 Inconel 718 English EUDocument9 pagesSDS 791471000 Inconel 718 English EUConstantin Romica StoicaNo ratings yet
- Shangrila 510S: Portable VentilatorDocument3 pagesShangrila 510S: Portable VentilatorAriefBukhari'abhi'No ratings yet
- Diaphragmatic Paralysis in Neonates with Brachial Plexus InjuryDocument3 pagesDiaphragmatic Paralysis in Neonates with Brachial Plexus InjuryDennyNo ratings yet
- DAN Tech Proceedings Feb2010Document396 pagesDAN Tech Proceedings Feb2010SerbanNo ratings yet
- Safety Data Sheet: Section 1. IdentificationDocument15 pagesSafety Data Sheet: Section 1. IdentificationIverson RegaladoNo ratings yet
- Health Week 1-3 - 3rd QuarterDocument8 pagesHealth Week 1-3 - 3rd QuarterNoemelyn VecinaNo ratings yet
- SYNOPSIS - Prevelance of FHP and Its Effect On Breathing Among Students of IIUI Final PDFDocument11 pagesSYNOPSIS - Prevelance of FHP and Its Effect On Breathing Among Students of IIUI Final PDFAli AfaqNo ratings yet
- Acute Conditions Requiring Oxygen TherapyDocument9 pagesAcute Conditions Requiring Oxygen TherapysukhmaniNo ratings yet
- Jurnal Skripsi Anestesi 4Document8 pagesJurnal Skripsi Anestesi 4Tiara Anggun NurartoNo ratings yet
- Pigment (1922)Document6 pagesPigment (1922)Waqar YounasNo ratings yet
- ARDSDocument1 pageARDSTito TesfayeNo ratings yet
- TYLER M. L. Pointers To The Common RemediesDocument224 pagesTYLER M. L. Pointers To The Common RemediesHasinYusuf100% (4)
- Interstitial Pneumonia With Autoimmune Features (IPAF) : Interesting CaseDocument10 pagesInterstitial Pneumonia With Autoimmune Features (IPAF) : Interesting CaseSilp SatjawattanavimolNo ratings yet