You might also like
- Elsye Gunawan: Farmakoterapi Pada Pasien MalariaDocument47 pagesElsye Gunawan: Farmakoterapi Pada Pasien MalariaEnvhy WinaNo ratings yet
- Management of Complicated MalariaDocument36 pagesManagement of Complicated MalariaAnu SinhaNo ratings yet
- Malaria MB CHB January 2018-FinalDocument36 pagesMalaria MB CHB January 2018-Finalokwadha simionNo ratings yet
- Consultant Physician, NDUTH: MBBS, FWACP, FMCP-Infectious DiseaseDocument46 pagesConsultant Physician, NDUTH: MBBS, FWACP, FMCP-Infectious DiseasePrincewill SeiyefaNo ratings yet
- Malaria: Dr. Harun Hudari, SPPDDocument49 pagesMalaria: Dr. Harun Hudari, SPPDEdvans HenryNo ratings yet
- Malaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaDocument27 pagesMalaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaAnonymous Di1zSIkRBHNo ratings yet
- GROUP A1 (A) Topic 5Document37 pagesGROUP A1 (A) Topic 5KhaiNo ratings yet
- Protozoal InfectionDocument66 pagesProtozoal InfectionGEM SCANNo ratings yet
- Antiparasitic Agents RevisedDocument94 pagesAntiparasitic Agents RevisedJe SantosNo ratings yet
- Malaria in PregnancyDocument28 pagesMalaria in PregnancyPeprah Ondiba100% (1)
- Uncomplicated Malaria and TreatmentDocument44 pagesUncomplicated Malaria and TreatmentSisilia AlfinaNo ratings yet
- Malaria: Department of Internal Medicine, School of MedicineDocument33 pagesMalaria: Department of Internal Medicine, School of MedicineAndarge ImperialNo ratings yet
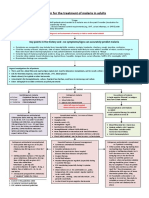
- Algorithm For The Treatment of Malaria in AdultsDocument1 pageAlgorithm For The Treatment of Malaria in AdultsRihab IsmaeelNo ratings yet
- Malaria: Presented By: Anish Dhakal (Aryan)Document31 pagesMalaria: Presented By: Anish Dhakal (Aryan)Ignatius Bayu HermawanNo ratings yet
- Malaria Lecture NoteDocument10 pagesMalaria Lecture NoteOKONKWO OBINNANo ratings yet
- SachinDocument36 pagesSachinapi-3741769100% (1)
- Case 3.2 (Malaria) : Arwa Hussain Al-Onayzan. 215007943. 66Document24 pagesCase 3.2 (Malaria) : Arwa Hussain Al-Onayzan. 215007943. 66Danial HassanNo ratings yet
- Malaria Es PregcyDocument61 pagesMalaria Es PregcyNinaNo ratings yet
- Malaria. Mr.r.phiriDocument29 pagesMalaria. Mr.r.phiricheweblessings03No ratings yet
- 1 - Uncomplicated Malaria and TreatmentDocument35 pages1 - Uncomplicated Malaria and Treatmentstivana26No ratings yet
- Management of Severe Malaria CasesDocument100 pagesManagement of Severe Malaria CasesAshis karmakarNo ratings yet
- Malaria 2012Document43 pagesMalaria 2012van_cristianoNo ratings yet
- Ringkasan Malaria: Agustin Iskandar, DR, Mkes, SPPKDocument35 pagesRingkasan Malaria: Agustin Iskandar, DR, Mkes, SPPKnisrinaNo ratings yet
- Travel Associated Infections: Sunanda Gaur, MDDocument49 pagesTravel Associated Infections: Sunanda Gaur, MDhernandez2812No ratings yet
- Malaria Dalam Kehamilan: Erni Juwita Nelwan Divisi Tropik Dan Penyakit Infeksi Fkui - RSCMDocument27 pagesMalaria Dalam Kehamilan: Erni Juwita Nelwan Divisi Tropik Dan Penyakit Infeksi Fkui - RSCMadrianamarshaNo ratings yet
- Epidemiology Prevention & Control of Malaria: Dr. Neha Tyagi Assistant Professor Department of Community MedicineDocument29 pagesEpidemiology Prevention & Control of Malaria: Dr. Neha Tyagi Assistant Professor Department of Community MedicineShashi TyagiNo ratings yet
- Vulvovaginal InfectionDocument66 pagesVulvovaginal InfectionRadhika BambhaniaNo ratings yet
- MalariaDocument44 pagesMalariasantosh goitNo ratings yet
- Malaria/Hms: Dr. Muhammad Hamza (MB, BS, FMCP) Department of Medicine Akth/Buk KanoDocument47 pagesMalaria/Hms: Dr. Muhammad Hamza (MB, BS, FMCP) Department of Medicine Akth/Buk Kanoadamu mohammadNo ratings yet
- Malaria: DR MD Mamunul Abedin ShimulDocument41 pagesMalaria: DR MD Mamunul Abedin ShimulDr. Mamunul AbedinNo ratings yet
- Malaria Epidemiology & Prevention: Group Captain AD Green Royal Centre For Defence MedicineDocument55 pagesMalaria Epidemiology & Prevention: Group Captain AD Green Royal Centre For Defence MedicineMohammed YaqoobNo ratings yet
- Materi Dr. Dr. Dominicus Husada, Sp.A (K) PDFDocument47 pagesMateri Dr. Dr. Dominicus Husada, Sp.A (K) PDFmahyarani dalimuntheNo ratings yet
- Kala Azar and LeptospirosisDocument36 pagesKala Azar and LeptospirosisAbhinav AggarwalNo ratings yet
- Arthropod Borne Infections - MHA (12 Files Merged)Document377 pagesArthropod Borne Infections - MHA (12 Files Merged)MariaNo ratings yet
- MALARIA (Autosaved)Document16 pagesMALARIA (Autosaved)Mpanso Ahmad AlhijjNo ratings yet
- 7 - Case - ParasiticDocument18 pages7 - Case - Parasitickoteshwara raoNo ratings yet
- Malaria 15.3.2022Document29 pagesMalaria 15.3.2022odhiambo samwelNo ratings yet
- Lascano, Joanne Alyssa H. - Parasitology SGDDocument8 pagesLascano, Joanne Alyssa H. - Parasitology SGDJoanne Alyssa Hernandez LascanoNo ratings yet
- Vector Borne Diseases: (Malaria)Document34 pagesVector Borne Diseases: (Malaria)Srinivas KasiNo ratings yet
- Antiprotozoal Drugs: Halia Wanadiatri, DR., M.SiDocument34 pagesAntiprotozoal Drugs: Halia Wanadiatri, DR., M.SiBaiqLinaAnggrianNo ratings yet
- Edited Monkeypox Facts 2022Document93 pagesEdited Monkeypox Facts 2022anghelmiguel07262016No ratings yet
- Microsoft PowerPoint - KNUST-LECT-STUDENT MALARIA (Compatibility Mode)Document9 pagesMicrosoft PowerPoint - KNUST-LECT-STUDENT MALARIA (Compatibility Mode)AnastasiafynnNo ratings yet
- MalariaDocument21 pagesMalariaRakshithNo ratings yet
- Malaria & Cerebral Malaria: Livia Hanisamurti, S.Ked 71 2018 045Document40 pagesMalaria & Cerebral Malaria: Livia Hanisamurti, S.Ked 71 2018 045Livia HanisamurtiNo ratings yet
- SEI - INEP - 0137469 - Projeto BásicoDocument29 pagesSEI - INEP - 0137469 - Projeto BásicoMARLOMbran HERRNo ratings yet
- Malaria in Pregnancy. NewDocument23 pagesMalaria in Pregnancy. Newgloriashirima8No ratings yet
- Malaria: Dr. Shree Narayan Yadav Internal Medicine Resident NamsDocument44 pagesMalaria: Dr. Shree Narayan Yadav Internal Medicine Resident Namsasyanadhikary18No ratings yet
- Malaria LectureDocument32 pagesMalaria LectureNwosu Ogbonna GabrielNo ratings yet
- MalariaDocument39 pagesMalariaUmi Chusnul Chotimah I100% (1)
- Candidiasis IDSA 2016Document23 pagesCandidiasis IDSA 2016Shihan HuqNo ratings yet
- Malaria by Dr. A.M IyagbaDocument51 pagesMalaria by Dr. A.M IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Management of Severe Malaria: Paul N HarijantoDocument56 pagesManagement of Severe Malaria: Paul N HarijantoDaniel MatiusNo ratings yet
- Malaria: Dr. Shree Narayan Yadav Internal Medicine Resident NamsDocument40 pagesMalaria: Dr. Shree Narayan Yadav Internal Medicine Resident Namsasyanadhikary18No ratings yet
- Severe Plasmodium Falciparum Malaria: Utility of Exchange TransfusionDocument11 pagesSevere Plasmodium Falciparum Malaria: Utility of Exchange TransfusionArja' WaasNo ratings yet
- Tropical Id UpdateDocument75 pagesTropical Id UpdateBalqis OktapNo ratings yet
- 06 Uncomplicated MalariaDocument16 pages06 Uncomplicated MalariaMwanja MosesNo ratings yet
- ANTIMALARIAL DrugsDocument25 pagesANTIMALARIAL DrugsMANAS ChhapoliyaNo ratings yet
- CH 25 Mycoplasma and UreaplasmaDocument14 pagesCH 25 Mycoplasma and UreaplasmashericeNo ratings yet
- Malaria 1Document20 pagesMalaria 1Ankush GahlotNo ratings yet