You might also like
- Sulphur Amino AcidsDocument23 pagesSulphur Amino Acidsmadhuribiswal7700No ratings yet
- BIO 202 Biochemistry II by Seyhun YURDUGÜL: Amino Acid Metabolism I: Amino Acid BiosynthesisDocument65 pagesBIO 202 Biochemistry II by Seyhun YURDUGÜL: Amino Acid Metabolism I: Amino Acid BiosynthesisYasin Çağrı KılıçerNo ratings yet
- Protein Turn OverDocument29 pagesProtein Turn Overabdullah zaheerNo ratings yet
- 4 Protein ReviewDocument87 pages4 Protein Reviewmika de guzmanNo ratings yet
- 3 Metabolism of Proteins & Amino AcidsDocument79 pages3 Metabolism of Proteins & Amino AcidsYashfa YasinNo ratings yet
- Metabolism of Amino AcidsDocument77 pagesMetabolism of Amino Acidswhpzm6ttg8No ratings yet
- Urea Cycle and Protein MetabolismDocument39 pagesUrea Cycle and Protein Metabolismikramullahkhan211No ratings yet
- Amino Acid Catabolism-Part-1: Biochemistry For Medics - Lecture Notes Professor (DR.) Namrata ChhabraDocument43 pagesAmino Acid Catabolism-Part-1: Biochemistry For Medics - Lecture Notes Professor (DR.) Namrata Chhabrashree devNo ratings yet
- UrineDocument41 pagesUrineWahab KhaniNo ratings yet
- Lect1 - 2017Document28 pagesLect1 - 2017George MakoriNo ratings yet
- Protein and Amino Acid MetabolismDocument32 pagesProtein and Amino Acid MetabolismVirag0% (1)
- Protein MetabolismDocument182 pagesProtein MetabolismSimra ZahidNo ratings yet
- Chapter X - Mechanism of Protein MetabolismDocument30 pagesChapter X - Mechanism of Protein MetabolismAngelo AngelesNo ratings yet
- Specialized Product Formed From - Met, Phe, Tyr.Document33 pagesSpecialized Product Formed From - Met, Phe, Tyr.Shivanand MaliNo ratings yet
- Proteins and Amino Acids Metabolism: Tahun Ajar 2016/2017Document47 pagesProteins and Amino Acids Metabolism: Tahun Ajar 2016/2017Aswar AyuNo ratings yet
- Introduction Amino Acid Matabolism and CatabolismDocument45 pagesIntroduction Amino Acid Matabolism and CatabolismAboubakar Moalim Mahad moh'd100% (1)
- Biochemistry: Dr. Dra. Trini Suryowati, MsDocument49 pagesBiochemistry: Dr. Dra. Trini Suryowati, MsDaud ParluhutanNo ratings yet
- Physical Properties of ProteinsDocument46 pagesPhysical Properties of ProteinsTasneem AhmedNo ratings yet
- Amino Acid Catabolism II: Dr. Mohammad AkramDocument19 pagesAmino Acid Catabolism II: Dr. Mohammad Akramapi-19824406No ratings yet
- Amino Acids Metabolism Final For Pharm 2014Document57 pagesAmino Acids Metabolism Final For Pharm 2014Getu LuchesaNo ratings yet
- BP U9d Protein MetabolismDocument80 pagesBP U9d Protein MetabolismChristian Angelo AgbunagNo ratings yet
- 0091 Nabeel Yousaf Biochemistry Final Term PpaerDocument19 pages0091 Nabeel Yousaf Biochemistry Final Term PpaerAbdullah MunawarNo ratings yet
- Metabolism of Other Amino Acids: GlycineDocument9 pagesMetabolism of Other Amino Acids: GlycineAsad AliNo ratings yet
- 1.15 Amino Acid MetabolismDocument16 pages1.15 Amino Acid MetabolismnkhomaslaterNo ratings yet
- 6 Proteins Their Digestion & AbsorptionsDocument18 pages6 Proteins Their Digestion & AbsorptionshodaNo ratings yet
- Proteins and Liver Function TestsDocument56 pagesProteins and Liver Function TestsjoanNo ratings yet
- Amino Acid MetabolismDocument29 pagesAmino Acid MetabolismERIAS TENYWANo ratings yet
- Protein Metabolism Dental and Physiotherapy Part 1Document17 pagesProtein Metabolism Dental and Physiotherapy Part 1Nada Atef KoraitemNo ratings yet
- Amino Acid Oxidation andDocument23 pagesAmino Acid Oxidation andRahma FauziahNo ratings yet
- Sulphur Containing AminoacidsDocument36 pagesSulphur Containing AminoacidsSaloni SaloniNo ratings yet
- Urea CycleDocument4 pagesUrea CycleKunal DuttaNo ratings yet
- 202synthesis of Nonessential Amino Acids - Lec 02 PDFDocument35 pages202synthesis of Nonessential Amino Acids - Lec 02 PDFnyasha chinyangaNo ratings yet
- Lecture 5 - Synthesis of Non-Essential AADocument17 pagesLecture 5 - Synthesis of Non-Essential AAciyace7849No ratings yet
- Investigation of Amino Acids DisordersDocument4 pagesInvestigation of Amino Acids Disorderskiedd_04100% (1)
- BIOSINTESIS PROTlanjutanDocument31 pagesBIOSINTESIS PROTlanjutanAprilikkaearlyNo ratings yet
- S1 Bioqui RenalDocument46 pagesS1 Bioqui RenalIsabela Cristina Verdugo SinibaldiNo ratings yet
- Amino Acid Metabolism: The Nitrogen Cycle and Nitrogen FixationDocument54 pagesAmino Acid Metabolism: The Nitrogen Cycle and Nitrogen FixationAlbert TandyNo ratings yet
- Chemical Pathology BS-MLT 5Th SemesterDocument36 pagesChemical Pathology BS-MLT 5Th SemesterMuhammad AbdullahNo ratings yet
- (Biochemistry) Onsite Assignment No8 - Group XDocument33 pages(Biochemistry) Onsite Assignment No8 - Group XV THNo ratings yet
- B. Katabolisme Asam Amino-1Document19 pagesB. Katabolisme Asam Amino-1M Sifal MaulanaNo ratings yet
- Digestion and Absorption of ProteinsDocument15 pagesDigestion and Absorption of ProteinsEng Matti Ur Rehman100% (1)
- METABOLISME ASAM AMINO Protein BiologiDocument31 pagesMETABOLISME ASAM AMINO Protein BiologiAxzchiuu :vNo ratings yet
- Protien and Urea CycleDocument33 pagesProtien and Urea CycleTAUQEER Ali shahNo ratings yet
- Urea CycleDocument4 pagesUrea Cycletfgrn7srtqNo ratings yet
- Metabolism of Individual Amino Acids and Biosynthesis ofDocument33 pagesMetabolism of Individual Amino Acids and Biosynthesis ofAboubakar Moalim Mahad moh'dNo ratings yet
- Urea Cycle LehningerDocument34 pagesUrea Cycle LehningerMohamadJamaludinNo ratings yet
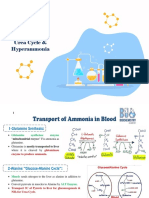
- Urea Cycle & HyperammoniaDocument6 pagesUrea Cycle & HyperammoniaSal TlsNo ratings yet
- Describe The Storage, Synthetic, Metabolic and Excretory Functions of The Liver and To Identify The Physiological Consequences of Hepatic DiseaseDocument15 pagesDescribe The Storage, Synthetic, Metabolic and Excretory Functions of The Liver and To Identify The Physiological Consequences of Hepatic DiseaseApril M WinNo ratings yet
- Biosynthesis and Degradation of Amino AcidsDocument22 pagesBiosynthesis and Degradation of Amino Acidsإضحك وبين سنانك Laugh and show your teethNo ratings yet
- Protein and Amino Acid MetabolismDocument52 pagesProtein and Amino Acid MetabolismRisky OpponentNo ratings yet
- Referat HepatitisDocument46 pagesReferat Hepatitismiss.JEJENo ratings yet
- Urea Cycle: Dr. Amro Yousef Al-AmlehDocument45 pagesUrea Cycle: Dr. Amro Yousef Al-AmlehDr. Amro YousefNo ratings yet
- Metabolism of Aminoacids 2Document68 pagesMetabolism of Aminoacids 2Mi PatelNo ratings yet
- Other Amino Acids Form Succinyl CoaDocument23 pagesOther Amino Acids Form Succinyl CoanyarieNo ratings yet
- Individual Amino Acid 2Document52 pagesIndividual Amino Acid 2Mai Elsayed OmaraNo ratings yet
- Amino Acid Metabolism NotesDocument152 pagesAmino Acid Metabolism NotesAkhilesh TiwariNo ratings yet
- Metabolism of ProteinsDocument50 pagesMetabolism of ProteinsAbdur RehmanNo ratings yet
- Amino Acids BiosynthesisDocument56 pagesAmino Acids BiosynthesisDeea LobonțiuNo ratings yet
- S G DDocument3 pagesS G Dt-oNo ratings yet
- Metabolism of Amino AcidsDocument91 pagesMetabolism of Amino AcidsAditya NayakNo ratings yet
- BCH103 7Document6 pagesBCH103 7PRATEEK KUMARNo ratings yet
- Molecules 28 04123Document28 pagesMolecules 28 04123Aura RusuNo ratings yet
- Unit 3 DeaminationDocument27 pagesUnit 3 DeaminationAsjad HassanNo ratings yet
- Biology Mnemonics For NEETDocument10 pagesBiology Mnemonics For NEETadarsh29adityaNo ratings yet
- CHM4116 Nitrogen Metab ReviewerDocument22 pagesCHM4116 Nitrogen Metab ReviewerBEA FRANCINE DELOS SANTOSNo ratings yet
- Pancreatic Cancer MetabolismDocument36 pagesPancreatic Cancer MetabolismShivaprakash Jagalur MuttNo ratings yet
- C10 Protein and Amino Acid MetabolismDocument8 pagesC10 Protein and Amino Acid MetabolismSoraya D. Al-ObinayNo ratings yet
- Amino Acid Metabolism NotesDocument37 pagesAmino Acid Metabolism NotesIbtisam DoughanNo ratings yet
- Amino Acid Metabolism All LecturesDocument18 pagesAmino Acid Metabolism All Lecturesmizare29gNo ratings yet
- Module 10 RationaleDocument3 pagesModule 10 RationaleG INo ratings yet