You might also like
- Pharmacology of Inotropes and VasopressorsDocument51 pagesPharmacology of Inotropes and VasopressorsApen Silaban100% (1)
- Pharmacology of Adrenergic AgonistsDocument9 pagesPharmacology of Adrenergic Agonistsfiena92No ratings yet
- INOTROPESDocument8 pagesINOTROPESessevyNo ratings yet
- Inotropes, Excellent Article, With DosingDocument47 pagesInotropes, Excellent Article, With DosingNavojit ChowdhuryNo ratings yet
- ACLS DrugDocument7 pagesACLS DrugPhongsatorn Thunin100% (1)
- Hemodynamic Drug InfusionsDocument45 pagesHemodynamic Drug InfusionsDawit MucheNo ratings yet
- Abdominal "Signs" Table: Sign Diagnosis/ConditionDocument1 pageAbdominal "Signs" Table: Sign Diagnosis/ConditionMeg AmoonNo ratings yet
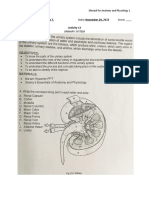
- Urinary SystemDocument5 pagesUrinary SystemJushelle Anne Tigoy Pilare100% (1)
- Adrenergic Agonist and AntagonistDocument35 pagesAdrenergic Agonist and AntagonistFirjat AfiataNo ratings yet
- VASOACTIVE THERAPY GUIDE FOR CRITICALLY ILL PATIENTSDocument26 pagesVASOACTIVE THERAPY GUIDE FOR CRITICALLY ILL PATIENTSlidya agustin100% (1)
- Pain ManagementDocument39 pagesPain Managementsteven saputra100% (1)
- Emergency Medications GuideDocument7 pagesEmergency Medications Guidejohn72decNo ratings yet
- Aherrera Notes PDFDocument213 pagesAherrera Notes PDFjampogaott100% (1)
- NCM 112 Midterm ExamDocument16 pagesNCM 112 Midterm ExamYman Gio BumanglagNo ratings yet
- Management of Shock: Role of Inotropic & Vasoactive DrugsDocument50 pagesManagement of Shock: Role of Inotropic & Vasoactive DrugsbajaocNo ratings yet
- Care of Clients with Respiratory ProblemsDocument115 pagesCare of Clients with Respiratory ProblemsarielleortuosteNo ratings yet
- INOTROPESDocument28 pagesINOTROPESsinghal297% (30)
- Term 3 Rationale Pharmacology and MCNDocument35 pagesTerm 3 Rationale Pharmacology and MCNKing KongNo ratings yet
- The rate of infusion is 15 mL/hrDocument48 pagesThe rate of infusion is 15 mL/hrUnihealth Southwoods NursingNo ratings yet
- Photosynthesis and Cellular Respiration AssessmentDocument8 pagesPhotosynthesis and Cellular Respiration Assessmentapi-489727615100% (1)
- Adrenaline (Epinephrine) : InotropesDocument4 pagesAdrenaline (Epinephrine) : Inotropespachino007No ratings yet
- Dopamine Drug StudyDocument3 pagesDopamine Drug StudyNicole Soo78% (9)
- Acute Myocardial InfarctionDocument35 pagesAcute Myocardial Infarctionvirnzrobz80% (10)
- The Role of Occupational Therapy in Cardiac RehabilitationDocument35 pagesThe Role of Occupational Therapy in Cardiac Rehabilitationsdsd100% (1)
- Drug Study CARDIODocument17 pagesDrug Study CARDIODiannetotz Morales100% (1)
- Ion Channels as Drug TargetsDocument71 pagesIon Channels as Drug TargetsQonita NitaNo ratings yet
- Farmakologi Obat VasopresorDocument25 pagesFarmakologi Obat Vasopresoralex_christian1992No ratings yet
- Physiology MCQ - RespiratoryDocument14 pagesPhysiology MCQ - RespiratoryJoseph95% (19)
- Dopamine Drug StudyDocument6 pagesDopamine Drug StudyGeorge RussellNo ratings yet
- Farmakologi Obat VasopresorDocument25 pagesFarmakologi Obat Vasopresorhendrik taufikNo ratings yet
- Farmakologi Obat VasopresorDocument25 pagesFarmakologi Obat VasopresorNudyan BetharinaNo ratings yet
- MedicationsDocument30 pagesMedicationsvamshidhNo ratings yet
- Vasopressors and Inotropes: Dobutamine, Dopamine, EpinephrineDocument100 pagesVasopressors and Inotropes: Dobutamine, Dopamine, EpinephrineMorad SatariNo ratings yet
- Inotropic in ICUDocument24 pagesInotropic in ICUAmira HelayelNo ratings yet
- SympathomimeticDocument56 pagesSympathomimeticvarish0% (1)
- SympatheticDocument10 pagesSympatheticSharneeshriyaNo ratings yet
- High AlertDocument61 pagesHigh Alertdrsidra.mustafaNo ratings yet
- The Use of Vasopressor and Inotropes in The Emergency Departement For The Treatment of ShockDocument36 pagesThe Use of Vasopressor and Inotropes in The Emergency Departement For The Treatment of ShockAndre Eka Putra PrakosaNo ratings yet
- Penggunaan Vasopresor Dan Inotropik Dalam Penanganan Darurat SYOK - .Document25 pagesPenggunaan Vasopresor Dan Inotropik Dalam Penanganan Darurat SYOK - .Habibullah AlNo ratings yet
- Critical Care Dr. Valerie Zarza GeronDocument88 pagesCritical Care Dr. Valerie Zarza GeronDivine Grace FernandezNo ratings yet
- Hypertensive Emergencies: BY: Dr. Imtiyaz Hashim (PGR) Dr. Khalida Baloch (Ho)Document31 pagesHypertensive Emergencies: BY: Dr. Imtiyaz Hashim (PGR) Dr. Khalida Baloch (Ho)امتیاز ہاشم بزنجوNo ratings yet
- Inotropes in PICU: Uses and Effects of Dopamine, Epinephrine, Dobutamine, Milrinone, Norepinephrine, and VasopressinDocument2 pagesInotropes in PICU: Uses and Effects of Dopamine, Epinephrine, Dobutamine, Milrinone, Norepinephrine, and VasopressinDijattxNo ratings yet
- Vasoactive TherapyDocument26 pagesVasoactive Therapylidya agustinNo ratings yet
- Epinephrine Dosage and AdministrationDocument9 pagesEpinephrine Dosage and AdministrationTushar GhuleNo ratings yet
- InotropicsDocument20 pagesInotropicsMalathi VarnaNo ratings yet
- Nstemi: ContraindicationsDocument8 pagesNstemi: ContraindicationsWita Ferani KartikaNo ratings yet
- INOTROPES AND VASOPRESSORS OVERVIEWDocument62 pagesINOTROPES AND VASOPRESSORS OVERVIEWtwister4No ratings yet
- Critical Care - UnitDocument80 pagesCritical Care - Unitsuganthi rajesh kanna100% (1)
- Heart Failure: Causes, Treatments, and Dental ImplicationsDocument8 pagesHeart Failure: Causes, Treatments, and Dental Implicationsمحمد علي حميدNo ratings yet
- GROUP3 Multiple-ChoiceDocument4 pagesGROUP3 Multiple-Choicelea mae andoloyNo ratings yet
- Vasoactive Medication Mmre (Autosaved)Document31 pagesVasoactive Medication Mmre (Autosaved)mohamed rashadNo ratings yet
- Antianginal Student222Document69 pagesAntianginal Student222MoonAIRNo ratings yet
- CARDIO Intensive CareDocument6 pagesCARDIO Intensive CareDianne Erika MeguinesNo ratings yet
- Classdrugtherapyofshock 160310043509Document55 pagesClassdrugtherapyofshock 160310043509febr1sNo ratings yet
- Emergency Drugs GuideDocument8 pagesEmergency Drugs GuideShehnaz SheikhNo ratings yet
- 8 IsoproterenolDocument8 pages8 IsoproterenolSilvia RNo ratings yet
- Drug StudyDocument7 pagesDrug StudydivineNo ratings yet
- INOTROPES by RavitejaDocument83 pagesINOTROPES by RavitejapriyadikkalaNo ratings yet
- FarmakologiDocument69 pagesFarmakologikekeyirawanNo ratings yet
- E Cart MedicationsDocument12 pagesE Cart Medicationsbalong1219No ratings yet
- Chapter - 015 Adrenergic Agonists and AntagonistsDocument52 pagesChapter - 015 Adrenergic Agonists and AntagonistsMaureen CuartoNo ratings yet
- Drug StudypppDocument42 pagesDrug Studyppp2022106284No ratings yet
- Adult and Pediatric Emergency DrugsDocument61 pagesAdult and Pediatric Emergency DrugsYu, Denise Kyla BernadetteNo ratings yet
- Update: Review and Update On Inotropes and VasopressorsDocument9 pagesUpdate: Review and Update On Inotropes and VasopressorsMaryam JamilahNo ratings yet
- Adrenergic Drugs Actions UsesDocument3 pagesAdrenergic Drugs Actions UsesRohit GodaseNo ratings yet
- 05-Adrenergic Agonists DR Hala 2020Document30 pages05-Adrenergic Agonists DR Hala 2020مشاعرمبعثرةNo ratings yet
- Adrenergic Drugs: S. Parasuraman, M.Pharm., PH.D.Document25 pagesAdrenergic Drugs: S. Parasuraman, M.Pharm., PH.D.Zakaria salimNo ratings yet
- Drugs Given During Cardiac Arres For CPRDocument5 pagesDrugs Given During Cardiac Arres For CPREevyaj MimiNo ratings yet
- L18 - Adrenergics IIIDocument10 pagesL18 - Adrenergics IIIyasaira707No ratings yet
- Diagram SWOT Analysis Chart TemplateDocument1 pageDiagram SWOT Analysis Chart TemplatejavajavuNo ratings yet
- CV Publish NEW 2016Document9 pagesCV Publish NEW 2016javajavuNo ratings yet
- Pediatric Ambulatory PDFDocument20 pagesPediatric Ambulatory PDFjavajavuNo ratings yet
- Blood Transfusion in Crtitical IllDocument43 pagesBlood Transfusion in Crtitical IllAris TamaNo ratings yet
- Monitoring PerioperatipDocument54 pagesMonitoring Perioperatipjavajavu100% (1)
- Antiseptic AgentsDocument23 pagesAntiseptic AgentsjavajavuNo ratings yet
- Pediatric Ambulatory PDFDocument20 pagesPediatric Ambulatory PDFjavajavuNo ratings yet
- Pediatric Ambulatory PDFDocument20 pagesPediatric Ambulatory PDFjavajavuNo ratings yet
- Blood Transfusion in Crtitical IllDocument43 pagesBlood Transfusion in Crtitical IllAris TamaNo ratings yet
- Airway ManagementDocument76 pagesAirway ManagementjavajavuNo ratings yet
- Rapid Sequence Intubation (RSI) Outside of The Operating Room in Children: Medications For Sedation and ParalysisDocument20 pagesRapid Sequence Intubation (RSI) Outside of The Operating Room in Children: Medications For Sedation and ParalysisLORENA ALEJANDRA RUIZ ARDILANo ratings yet
- Seminar on Myocardial InfarctionDocument17 pagesSeminar on Myocardial InfarctionSuhas IngaleNo ratings yet
- The Muscular System ExplainedDocument46 pagesThe Muscular System ExplainedMonico SalangusteNo ratings yet
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungDocument47 pagesKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiNo ratings yet
- ESH-IP 2010 Validation of OMRON EVOLV (HEM-7600 T-E) v2Document11 pagesESH-IP 2010 Validation of OMRON EVOLV (HEM-7600 T-E) v2Pub PleNo ratings yet
- Biol 1610 Photosynthesis Worksheet Key ConceptsDocument2 pagesBiol 1610 Photosynthesis Worksheet Key ConceptsLindsey TamlinNo ratings yet
- Diagnosis and Management of Pulmonary EmbolismDocument17 pagesDiagnosis and Management of Pulmonary EmbolismHGZ1 RESIDENTESNo ratings yet
- 2022-23 F3 Biology Exam Mock Paper 1 1Document20 pages2022-23 F3 Biology Exam Mock Paper 1 1azuryicerobloxNo ratings yet
- Hematology: Mohamad H Qari, MD, FRCPADocument49 pagesHematology: Mohamad H Qari, MD, FRCPASantoz ArieNo ratings yet
- Unstable Angina: DR Abdul Mateen Ansari, MD Professor and HOD General Medicine, Cimsh, LucknowDocument27 pagesUnstable Angina: DR Abdul Mateen Ansari, MD Professor and HOD General Medicine, Cimsh, LucknowCyntia KhairaniNo ratings yet
- Anatomy of The Lymphatic SystemDocument76 pagesAnatomy of The Lymphatic SystemManisha RaoNo ratings yet
- UFS Mid-Year Exam Paper 1Document8 pagesUFS Mid-Year Exam Paper 1TsholofeloNo ratings yet
- Control and Coordination: Chapter - 7Document9 pagesControl and Coordination: Chapter - 7milind dhamaniya100% (1)
- Chapter 10Document3 pagesChapter 10Zoe DorothyNo ratings yet
- Anatomy of A Young Dicot RootDocument3 pagesAnatomy of A Young Dicot RootVanessa Leuterio0% (2)
- Initial Assessment: - Rambam Medical Center - DR Nordkin DmitriDocument60 pagesInitial Assessment: - Rambam Medical Center - DR Nordkin Dmitridheviant12No ratings yet
- Leaves OkDocument2 pagesLeaves OkHarrivcha W.SNo ratings yet
- Glycolysis CrosswordDocument1 pageGlycolysis Crosswordapi-405259496No ratings yet
- Template CVDocument4 pagesTemplate CVNurul FaikaNo ratings yet
- Stress Symptoms ChecklistDocument2 pagesStress Symptoms ChecklistEdgar ManubagNo ratings yet