You might also like
- Alcoholic Liver DiseaseDocument27 pagesAlcoholic Liver DiseaseIsaac MwangiNo ratings yet
- Drug Induced Liver Diseases (DILD) : M. DeepalakshmiDocument22 pagesDrug Induced Liver Diseases (DILD) : M. DeepalakshmicrissNo ratings yet
- Non Viral HepatitisDocument40 pagesNon Viral Hepatitisostaz2000100% (1)
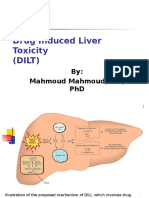
- Drug Induced Liver Toxicity-FinalDocument39 pagesDrug Induced Liver Toxicity-FinalAjeng SekariniNo ratings yet
- Alcoholic Liver Disease A Comprehensive Review1Document9 pagesAlcoholic Liver Disease A Comprehensive Review1Durga MadhuriNo ratings yet
- Chronic Liver Disease (Tutorial)Document44 pagesChronic Liver Disease (Tutorial)Hannah HalimNo ratings yet
- Approach To TransaminitisDocument20 pagesApproach To Transaminitisparik2321No ratings yet
- Lectu RioDocument7 pagesLectu RioTselmeg TselmegNo ratings yet
- Chemotherapy and Renal Andhepatic Insufficiency 2008Document24 pagesChemotherapy and Renal Andhepatic Insufficiency 2008Vika RatuNo ratings yet
- Evaluation of Abnormal Liver Function Tests: DR Chris Hovell Consultant Gastroenterologist Dorset County HospitalDocument59 pagesEvaluation of Abnormal Liver Function Tests: DR Chris Hovell Consultant Gastroenterologist Dorset County HospitalSaad MotawéaNo ratings yet
- Liver DiagnosticsDocument10 pagesLiver DiagnosticsTiny Briones-SallomanNo ratings yet
- Alcoholic Liver Disease - StatPearls - NCBI BookshelfDocument10 pagesAlcoholic Liver Disease - StatPearls - NCBI Bookshelfd99452727No ratings yet
- Alcohol and Anaesthesia - BJA Education - Oxford AcademicDocument14 pagesAlcohol and Anaesthesia - BJA Education - Oxford Academicayesha shaikNo ratings yet
- Alcoholic Liver Disease HarrisonDocument3 pagesAlcoholic Liver Disease HarrisonJesly Charlies0% (1)
- Liver CirhosisDocument15 pagesLiver CirhosisMoslem abd alzahra aziz AlsialwyNo ratings yet
- Chronic Liver Disease and CirrhosisDocument5 pagesChronic Liver Disease and Cirrhosisaqil ithninNo ratings yet
- Drug Induced Liver DiseaseDocument15 pagesDrug Induced Liver DiseaseMUGHALNo ratings yet
- CH 16 PDFDocument2 pagesCH 16 PDFKgerbNo ratings yet
- Liver Function Test 2011Document26 pagesLiver Function Test 2011anisa rachmitaNo ratings yet
- 2022-OXFORD-HANDBOOK-OF-ANAESTHESIA-Oxford-Press-5th-Edition ExportDocument3 pages2022-OXFORD-HANDBOOK-OF-ANAESTHESIA-Oxford-Press-5th-Edition ExportHany ElbarougyNo ratings yet
- Alcoholic Liver Disease: Last Updated: January 19, 2024Document16 pagesAlcoholic Liver Disease: Last Updated: January 19, 2024Tselmeg TselmegNo ratings yet
- Anesthesiaforliver Transplantation: Dieter Adelmann,, Kate Kronish,, Michael A. RamsayDocument18 pagesAnesthesiaforliver Transplantation: Dieter Adelmann,, Kate Kronish,, Michael A. RamsayJZNo ratings yet
- Ald 180226073505Document39 pagesAld 180226073505TianKaunangNo ratings yet
- LECTURES Liver PathophysiologyDocument118 pagesLECTURES Liver PathophysiologyTarik100% (1)
- ALD ReviewDocument8 pagesALD ReviewtcroscaNo ratings yet
- Liver - Systemic DiseasesDocument14 pagesLiver - Systemic Diseasessara.sherif099No ratings yet
- Acute Hepatic Failure: Dr. Idit Segal December 2003Document25 pagesAcute Hepatic Failure: Dr. Idit Segal December 2003ZeusKimNo ratings yet
- Abnormal Clinical Chemistry & TDM in CancerDocument44 pagesAbnormal Clinical Chemistry & TDM in CancerkinjalkaNo ratings yet
- Reviews: Alcoholic Liver Disease: Mechanisms of Injury and Targeted TreatmentDocument12 pagesReviews: Alcoholic Liver Disease: Mechanisms of Injury and Targeted TreatmentsilviahuesosNo ratings yet
- Alcoholic Liver Disease: DR Anigbo G E Consultant Physician/GastroenterologistDocument50 pagesAlcoholic Liver Disease: DR Anigbo G E Consultant Physician/GastroenterologistEbuka AniNo ratings yet
- Drug Induced Liver DisordersDocument31 pagesDrug Induced Liver DisordersJason fernandes jNo ratings yet
- Farmakologi Enterohepatal: Noor WijayahadiDocument134 pagesFarmakologi Enterohepatal: Noor WijayahadiYuni IsmulyatiNo ratings yet
- Hipertransaminasemia Com Marcadores Virales NegativosDocument17 pagesHipertransaminasemia Com Marcadores Virales NegativosJAvier Rodriguez-VeraNo ratings yet
- A Case of Liver Cirrhosis & Hepatic EncephalopathyDocument21 pagesA Case of Liver Cirrhosis & Hepatic EncephalopathyUdayakumar MannangattiNo ratings yet
- Interpretación Del Perfil HepáticoDocument10 pagesInterpretación Del Perfil HepáticoEdwin AlvarezNo ratings yet
- Acute Renal FailureDocument33 pagesAcute Renal Failureimranqazi11No ratings yet
- 340 Final StudyDocument21 pages340 Final StudyLeah ElizabethNo ratings yet
- Mq1 Liver Tumor DomantayDocument10 pagesMq1 Liver Tumor DomantayFroi Jovanni PerezNo ratings yet
- The Correlation of Transaminases and Liver DiseasesDocument11 pagesThe Correlation of Transaminases and Liver DiseasesFahni IndriyaniNo ratings yet
- Acute Liver FailureDocument3 pagesAcute Liver FailureElisabeth F. OjhaNo ratings yet
- Ald & MasldDocument19 pagesAld & MasldAli SafaaNo ratings yet
- Drug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineDocument21 pagesDrug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineAtakan Yeşil100% (1)
- Alcoholic Liver DiseaseDocument60 pagesAlcoholic Liver Diseasegarychia100% (1)
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaDocument36 pagesATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- Hepatotoxic DrugsDocument17 pagesHepatotoxic Drugsani bandasoNo ratings yet
- Non-Alcoholic Steatohepatitis (Nash) : Azzaki AbubakarDocument22 pagesNon-Alcoholic Steatohepatitis (Nash) : Azzaki AbubakarAdinda Suci MaghfiraNo ratings yet
- Liver Lab Essentials Liver Lab Essentials: Amer Wahed, MDDocument53 pagesLiver Lab Essentials Liver Lab Essentials: Amer Wahed, MDAbdulrahman M AlharbiNo ratings yet
- Alcoholic Liver DiseaseDocument32 pagesAlcoholic Liver Diseaseasamkele07No ratings yet
- Welcome To Journal Club Presentation: Presented byDocument54 pagesWelcome To Journal Club Presentation: Presented byneptorNo ratings yet
- Pathophysiology of Acute Liver FailureDocument39 pagesPathophysiology of Acute Liver Failurelefebi6403No ratings yet
- Drug Induced Liver InjuryDocument13 pagesDrug Induced Liver InjuryIhsan PutraNo ratings yet
- Drug Induced Liver Toxicity (DILD)Document39 pagesDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- Interactive Clinical Module 7ADocument13 pagesInteractive Clinical Module 7AKenedila MatetaNo ratings yet
- Phenelzine - Liver ToxicityDocument8 pagesPhenelzine - Liver Toxicitydo leeNo ratings yet
- Physiopathology 8Document4 pagesPhysiopathology 8I FNo ratings yet
- MODERATOR: Dr. Seraj A. Khan RESOURCE FACULTY: Dr. Smriti Karki PRESENTER: Deepa ChaudharyDocument20 pagesMODERATOR: Dr. Seraj A. Khan RESOURCE FACULTY: Dr. Smriti Karki PRESENTER: Deepa ChaudharyMadhusudan MadhavNo ratings yet
- AddisonsdiseaseDocument5 pagesAddisonsdiseasenessimmounir1173No ratings yet
- Fatty Liver AssignmentDocument9 pagesFatty Liver AssignmentMaryam ShahzadiNo ratings yet
- ACG Clinical Guideline Alcoholic Liver Disease.9Document20 pagesACG Clinical Guideline Alcoholic Liver Disease.9Gopal Kumar DasNo ratings yet
- Alcoholic Liver DiseaseDocument1 pageAlcoholic Liver DiseaseMin MawNo ratings yet
- GIT and LiverDocument28 pagesGIT and LiverUsmanNo ratings yet
- Etiologi Dan Patogenesis Ikterus,...Document103 pagesEtiologi Dan Patogenesis Ikterus,...Raditya PrimaNo ratings yet
- LECTURES Liver PathophysiologyDocument118 pagesLECTURES Liver PathophysiologyTarik100% (1)
- Pathophysiology of Alcoholic Liver DiseaseDocument4 pagesPathophysiology of Alcoholic Liver Diseaseshailendra tripathiNo ratings yet
- Alcoholic Hepatitis: A ReviewDocument9 pagesAlcoholic Hepatitis: A ReviewTugasbu CicikNo ratings yet
- Edited HP I Fri ConfDocument85 pagesEdited HP I Fri ConfTara Oliveros Dela CruzNo ratings yet
- Alcoholic Liver DiseaseDocument9 pagesAlcoholic Liver DiseasePankaj DixitNo ratings yet
- Pathology of Alcoholic Liver DiseaseDocument7 pagesPathology of Alcoholic Liver DiseasehghNo ratings yet
- Stages of Alcohol-Related Liver DiseaseDocument11 pagesStages of Alcohol-Related Liver DiseaseAF KoasNo ratings yet
- Liver Function TestDocument19 pagesLiver Function TestwertyuiNo ratings yet
- Alcohol Liver DiseaseDocument7 pagesAlcohol Liver DiseaseRavi ShankarNo ratings yet
- Assessment and Management of Oral Health in Liver Transplant CandidatesDocument5 pagesAssessment and Management of Oral Health in Liver Transplant Candidateswahyudi_donnyNo ratings yet
- Alcoholic Liver DiseaseDocument22 pagesAlcoholic Liver DiseaseVikramjeet SinghNo ratings yet
- Article Wjpps 15465140481Document12 pagesArticle Wjpps 15465140481Tech RajaNo ratings yet
- StringDocument3,369 pagesStringpractisemadhuriNo ratings yet
- Alcoholic Liver DiseaseDocument10 pagesAlcoholic Liver DiseaseNishanth ReddyNo ratings yet
- Acute Alcoholic HepatitisDocument18 pagesAcute Alcoholic HepatitisMariana NavarroNo ratings yet
- CP - Liver CirrhosisDocument161 pagesCP - Liver CirrhosisRomeo ReyesNo ratings yet
- Alcoholic Liver DiseaseDocument3 pagesAlcoholic Liver DiseaseEglNo ratings yet
- Cirrohsis and Alcoholic Liver DiseaseDocument8 pagesCirrohsis and Alcoholic Liver DiseaseZain Ul AbidinNo ratings yet
- Silymarin PharmacologyDocument18 pagesSilymarin PharmacologySilky Pradeep KumarNo ratings yet
- Alcoholic Liver DiseaseDocument8 pagesAlcoholic Liver DiseaseCassandra ZubeheourNo ratings yet
- ILC 2022 Abstract Book 08.06.2022Document1,104 pagesILC 2022 Abstract Book 08.06.2022Helena AlvesNo ratings yet
- Abnormal Liver Function TestsDocument6 pagesAbnormal Liver Function Testskronic12daniNo ratings yet
- Hepatic SteatosisDocument9 pagesHepatic Steatosiss12144017No ratings yet
- Enfermedad Hepática Por Alcohol: Alcoholic Liver DiseaseDocument13 pagesEnfermedad Hepática Por Alcohol: Alcoholic Liver DiseaseasierrNo ratings yet
- OSCE Case Practice 1: Pathology Station Marking Schemes: Well Done Partially Done Not DoneDocument5 pagesOSCE Case Practice 1: Pathology Station Marking Schemes: Well Done Partially Done Not DoneIsaac OngNo ratings yet