You might also like
- 8.1. Iron Deficiency AnemiaDocument39 pages8.1. Iron Deficiency AnemiaMichellyTjoaNo ratings yet
- Iron Deficiency Anemia: Causes, Symptoms and TreatmentDocument20 pagesIron Deficiency Anemia: Causes, Symptoms and TreatmentChingHuaNo ratings yet
- Dr. Haryanto - Kuliah Anemi Deff Fe 2011Document20 pagesDr. Haryanto - Kuliah Anemi Deff Fe 2011YeniNo ratings yet
- Iron Deficiency Anaemia: DR Mrs Stella Kanu Bmls Mbbs MSCDocument17 pagesIron Deficiency Anaemia: DR Mrs Stella Kanu Bmls Mbbs MSCDavid KanuNo ratings yet
- Recent IdaDocument30 pagesRecent IdaKashan SiddiquiNo ratings yet
- Nutrion Terapi of AnemiaDocument4 pagesNutrion Terapi of AnemiaRian LianNo ratings yet
- 6 Iron Deficiency AnemiaDocument3 pages6 Iron Deficiency AnemiaMelita SabellinaNo ratings yet
- AnemiaDocument37 pagesAnemiadr.umme habibaNo ratings yet
- Week 9 Anemia Part II - Microcytic and Macrocytic Anemia_revised - Copy-3Document6 pagesWeek 9 Anemia Part II - Microcytic and Macrocytic Anemia_revised - Copy-3Yoodge YoodgeNo ratings yet
- Nutritional Anemia: Dr. Mardiana, M.Kes, SP - GK Department of Clinical Nutrition Hasanuddin University MakassarDocument77 pagesNutritional Anemia: Dr. Mardiana, M.Kes, SP - GK Department of Clinical Nutrition Hasanuddin University MakassarDianaNo ratings yet
- Causes, Symptoms and Treatment of Iron-Deficiency AnemiaDocument17 pagesCauses, Symptoms and Treatment of Iron-Deficiency AnemiaEngland Dan EstacionNo ratings yet
- Join our Telegram channel for iron deficiency anemiaDocument12 pagesJoin our Telegram channel for iron deficiency anemiaKirubel DeribNo ratings yet
- Iron Deficiency and Iron OverloadDocument9 pagesIron Deficiency and Iron Overloadkat9210No ratings yet
- Drugs Acting On Blood and Blood Forming AgentsDocument29 pagesDrugs Acting On Blood and Blood Forming AgentsSri RamNo ratings yet
- 55.iron Def AnemiaDocument33 pages55.iron Def AnemiaMaria AlwanNo ratings yet
- The Role of Iron: Ahmad Sh. Silmi MSC Haematology, FIBMSDocument66 pagesThe Role of Iron: Ahmad Sh. Silmi MSC Haematology, FIBMSMohamed MidoNo ratings yet
- Hemtopoitic DrugDocument52 pagesHemtopoitic DrugUkash AbrahimNo ratings yet
- Copper Metabolism: Distribution of Copper in The BodyDocument4 pagesCopper Metabolism: Distribution of Copper in The BodyMichael HiiNo ratings yet
- Nutritional Anemia GuideDocument78 pagesNutritional Anemia GuideJoUng DjelauNo ratings yet
- Nutritional Therapy For Deficiency AnemiasDocument49 pagesNutritional Therapy For Deficiency AnemiasKartikaPANo ratings yet
- Iron Deficiency Anaemia (IDA) Diagnosis: Dr. Saifeldein M. A. ElimamDocument33 pagesIron Deficiency Anaemia (IDA) Diagnosis: Dr. Saifeldein M. A. ElimamSaifeldein ElimamNo ratings yet
- Chapter 3 NotesDocument10 pagesChapter 3 Notesmjamie12345No ratings yet
- Hematinics (Iron and Vitamin B12)Document53 pagesHematinics (Iron and Vitamin B12)shareksultan5No ratings yet
- Clinical Hematological: Assist Prof. Dr. Mudhir S. ShekhaDocument31 pagesClinical Hematological: Assist Prof. Dr. Mudhir S. ShekhaAhmed. Masud.OthmanNo ratings yet
- Hypochromic AnemiasDocument51 pagesHypochromic AnemiasKaylee NesbitNo ratings yet
- Iron Deficiency Anemia Lab Diagnosis and PathophysiologyDocument69 pagesIron Deficiency Anemia Lab Diagnosis and Pathophysiologyswathi bsNo ratings yet
- Iron Deficiency Anemia GeneticsDocument21 pagesIron Deficiency Anemia GeneticsTammy BoudNo ratings yet
- Iron Deficiency Anemia - An OverviewDocument6 pagesIron Deficiency Anemia - An OverviewIJAR JOURNALNo ratings yet
- Iron Def ADocument20 pagesIron Def Aacs.pathNo ratings yet
- Iron Deficiency AnemiaDocument88 pagesIron Deficiency AnemiaAbubakar JallohNo ratings yet
- Deficient, and 30% of This Group Progresses To Iron-Deficiency AnemiaDocument5 pagesDeficient, and 30% of This Group Progresses To Iron-Deficiency AnemiaTaeyomiNo ratings yet
- Anaemia Types and CausesDocument10 pagesAnaemia Types and CausesRazib HasanNo ratings yet
- Hepcidin's Role in Iron Distribution and Anemia of Chronic Kidney DiseaseDocument7 pagesHepcidin's Role in Iron Distribution and Anemia of Chronic Kidney DiseasegigibesiNo ratings yet
- Presentation 1Document100 pagesPresentation 1yukisam1318No ratings yet
- Hematological DiseasesDocument23 pagesHematological Diseasesmehnoor kaurNo ratings yet
- Anemia and Hematologic Drugs - KatzungDocument4 pagesAnemia and Hematologic Drugs - Katzungsarguss14100% (1)
- Anemia 1Document41 pagesAnemia 1julie kiskuNo ratings yet
- Nutritional AnemiaDocument55 pagesNutritional AnemiaL3mi DNo ratings yet
- Chemistry of Minerals-IIDocument29 pagesChemistry of Minerals-IIȘudîpțo ȘhăhîdNo ratings yet
- Chemistry of Minerals-IIDocument29 pagesChemistry of Minerals-IIȘudîpțo ȘhăhîdNo ratings yet
- IRON DEFICIENCY ANEMIADocument33 pagesIRON DEFICIENCY ANEMIAHatta Diana TariganNo ratings yet
- Iron Deficiency Anemia: Imran Shahzad Anjum, MDDocument38 pagesIron Deficiency Anemia: Imran Shahzad Anjum, MDshravaniNo ratings yet
- The Pharmacology of Iron: Absorption, Transport, and SupplementationDocument38 pagesThe Pharmacology of Iron: Absorption, Transport, and SupplementationSalmaNo ratings yet
- Iron Deficiency AnemiaDocument28 pagesIron Deficiency AnemiaKashan SiddiquiNo ratings yet
- Iron Deficiency AnemiaDocument24 pagesIron Deficiency AnemiaKailash KhatriNo ratings yet
- Лекция №2АнемииDocument16 pagesЛекция №2Анемии772footballNo ratings yet
- By: Dinsy Paul Juliet James Priya K Sravan Kumar. Potturi Govinda AjmeraDocument78 pagesBy: Dinsy Paul Juliet James Priya K Sravan Kumar. Potturi Govinda Ajmerashameer muhammedNo ratings yet
- Essential Trace ElementsDocument58 pagesEssential Trace ElementsrNo ratings yet
- Treatment of Anemia - No VidDocument69 pagesTreatment of Anemia - No Vidsylvia haryantoNo ratings yet
- Iron Deficiency Anemia GuideDocument13 pagesIron Deficiency Anemia GuidearbazNo ratings yet
- 3 - Iron Deficiency Anemia + ACD+Abnormal Heme SynthesisDocument101 pages3 - Iron Deficiency Anemia + ACD+Abnormal Heme SynthesisMotasem ZahaykaNo ratings yet
- Drugs Used in The Treatment of Anemia: Prepared By: Dr. Ghazi BamagousDocument42 pagesDrugs Used in The Treatment of Anemia: Prepared By: Dr. Ghazi BamagousAyman B-DadyNo ratings yet
- IronDocument18 pagesIronAbeer BasharatNo ratings yet
- Understanding Iron Metabolism and its Role in Health and DiseaseDocument24 pagesUnderstanding Iron Metabolism and its Role in Health and DiseaseShweta IyerNo ratings yet
- Iron Deficiency AnemiaDocument13 pagesIron Deficiency AnemiaRommel IsraelNo ratings yet
- Chapter 20 HemaDocument9 pagesChapter 20 HemaEMETERIO TUTOR IIINo ratings yet
- Haematopoietic Agents & Erythropoeitin: Dr. Rishi Pal Assistant Professor Department of PharmacologyDocument43 pagesHaematopoietic Agents & Erythropoeitin: Dr. Rishi Pal Assistant Professor Department of PharmacologyDERRICK AAGYEREYIR SAANUMENo ratings yet
- Iron Deficiency AnemiaDocument17 pagesIron Deficiency Anemiaمصطفى عبد الرزاق ورد حسينNo ratings yet
- Iron's Role in Hemoglobin and Myoglobin CyclesDocument45 pagesIron's Role in Hemoglobin and Myoglobin CyclesnajwaNo ratings yet
- A Simple Guide to Anemia, Treatment and Related DiseasesFrom EverandA Simple Guide to Anemia, Treatment and Related DiseasesRating: 4.5 out of 5 stars4.5/5 (2)
- Mixing Water Requirements for ConcreteDocument8 pagesMixing Water Requirements for ConcreteElvis Santillán CórdovaNo ratings yet
- Microsoft Word - Section 2 - Acid AdditivesDocument25 pagesMicrosoft Word - Section 2 - Acid AdditivesCynthy Ivonne Torres PerezNo ratings yet
- Industrial Craft GuideDocument56 pagesIndustrial Craft GuideCarrington Henley67% (6)
- Thermodynamic Constraints of Slag FormationDocument4 pagesThermodynamic Constraints of Slag FormationPinNo ratings yet
- What is cast iron? Key properties and typesDocument27 pagesWhat is cast iron? Key properties and typesSanthoshsharma Devaraju100% (1)
- Residual Stresses in Iron: CastingsDocument37 pagesResidual Stresses in Iron: CastingsAdityaNo ratings yet
- "Facts Are Not Science - As The Dictionary Is Not Literature." Martin H. FischerDocument16 pages"Facts Are Not Science - As The Dictionary Is Not Literature." Martin H. FischerVivek TripathyNo ratings yet
- 9.tubing SpecificationsDocument1 page9.tubing SpecificationsRaag SNo ratings yet
- A. Atoms: Engineering MaterialsDocument36 pagesA. Atoms: Engineering MaterialsAmpolNo ratings yet
- Unit 9 - Metals and Their Compounds Teacher VersionDocument29 pagesUnit 9 - Metals and Their Compounds Teacher VersionAmadu sallieuNo ratings yet
- Verrier Elwin, Sarat Chandra Roy - The Agaria (1992, Oxford University Press, USA)Document383 pagesVerrier Elwin, Sarat Chandra Roy - The Agaria (1992, Oxford University Press, USA)ravibaswaniNo ratings yet
- Civil Vi Environmental Engineering I (10cv61) SolutionDocument60 pagesCivil Vi Environmental Engineering I (10cv61) SolutionMithesh KumarNo ratings yet
- Fisa Purolite MZ 10 - EngDocument5 pagesFisa Purolite MZ 10 - EngTudor TaranuNo ratings yet
- JAMB Chemistry Past Question 1983 2004Document119 pagesJAMB Chemistry Past Question 1983 2004iamprecious2allNo ratings yet
- (Morgan, John H) Cathodic Protection (B-Ok - Xyz)Document567 pages(Morgan, John H) Cathodic Protection (B-Ok - Xyz)Shubhodeep SarkarNo ratings yet
- Material Grade Comparison TableDocument6 pagesMaterial Grade Comparison TableGhazali Zuberi100% (3)
- Cell Salt Kali PhosDocument34 pagesCell Salt Kali PhosPujari Ankur100% (3)
- Material Balance & Process Flow Sheet of PlantDocument13 pagesMaterial Balance & Process Flow Sheet of PlantAnkit AswalNo ratings yet
- The Company Profile PDFDocument10 pagesThe Company Profile PDFAnonymous jSv08eNo ratings yet
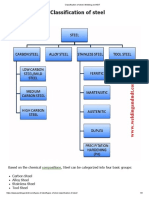
- Classification of Steel - Welding and NDTDocument3 pagesClassification of Steel - Welding and NDTAshif Iqubal100% (1)
- ASTM D943-04a - Oxidation of Inhibited Mineral OilDocument10 pagesASTM D943-04a - Oxidation of Inhibited Mineral OilKamruzaman MiahNo ratings yet
- Dear SirDocument12 pagesDear SirdjancoqueNo ratings yet
- 04Cr18Ni10 PDFDocument3 pages04Cr18Ni10 PDFAvishekNo ratings yet
- Ee 1919 08Document96 pagesEe 1919 08Akram KareemNo ratings yet
- Kenna MetalDocument2 pagesKenna MetalArshadAliNo ratings yet
- Nanosecond Electromagnetic Pulse Effect On Phase CompositionDocument8 pagesNanosecond Electromagnetic Pulse Effect On Phase CompositionAKNo ratings yet
- CHEM 142 Experiment #4: Calibration Curves and An Application of Beer's LawDocument4 pagesCHEM 142 Experiment #4: Calibration Curves and An Application of Beer's LawMakiaNo ratings yet
- Analysis of soil nutrient levels in coffee farmsDocument5 pagesAnalysis of soil nutrient levels in coffee farmsAbisai SanchezNo ratings yet
- Mech 340-HW4Document4 pagesMech 340-HW4sridndNo ratings yet
- ASTM A536 - 84 (2019) E1 Especificación Estándar para Fundiciones de Hierro DúctilDocument5 pagesASTM A536 - 84 (2019) E1 Especificación Estándar para Fundiciones de Hierro DúctilEder Rys100% (1)