You might also like
- Cat 3056 EDocument166 pagesCat 3056 EFranco Mayanga100% (8)
- 1 Peter GNT by Kenneth S WuestDocument61 pages1 Peter GNT by Kenneth S WuestMartha E. Ayala80% (5)
- ACLS PharmacologyDocument6 pagesACLS PharmacologyEunice Angela Fulgueras83% (6)
- Practice Reflection Worksheet Jithesh VKDocument3 pagesPractice Reflection Worksheet Jithesh VKapi-353376334100% (2)
- Critical Care - UnitDocument80 pagesCritical Care - Unitsuganthi rajesh kanna100% (1)
- ACLS MedicationsDocument31 pagesACLS MedicationscmirceaNo ratings yet
- Core Criteria Nov11Document3 pagesCore Criteria Nov11parents021No ratings yet
- St. John PassionDocument17 pagesSt. John PassionRafael BianchinNo ratings yet
- Bajaj Cash Assure Renewal Receipt PDFDocument1 pageBajaj Cash Assure Renewal Receipt PDFPawan KumarNo ratings yet
- 15 - CCLS - PharmacologyDocument32 pages15 - CCLS - PharmacologyVENKATESH RAMSALINo ratings yet
- Cardiovascular Pharmacology: DR Muhamad Ali Sheikh Abdul Kader MD (Usm) MRCP (Uk) Cardiologist, Penang HospitalDocument63 pagesCardiovascular Pharmacology: DR Muhamad Ali Sheikh Abdul Kader MD (Usm) MRCP (Uk) Cardiologist, Penang HospitalCvt RasulNo ratings yet
- Resuscitation Pharmacology: Dr. Beny Hartono, SPJP, FihaDocument44 pagesResuscitation Pharmacology: Dr. Beny Hartono, SPJP, FihaAna AgustinaNo ratings yet
- Critical Care Dr. Valerie Zarza GeronDocument88 pagesCritical Care Dr. Valerie Zarza GeronDivine Grace FernandezNo ratings yet
- High AlertDocument61 pagesHigh Alertdrsidra.mustafaNo ratings yet
- Management Strategy in Hypertensive Crisis The Role of NicardipineDocument38 pagesManagement Strategy in Hypertensive Crisis The Role of Nicardipinezulfikar adiNo ratings yet
- Hemodynamic Drug InfusionsDocument45 pagesHemodynamic Drug InfusionsDawit MucheNo ratings yet
- ACE InhibitorsDocument25 pagesACE InhibitorsShihab AlmoliukiNo ratings yet
- Anti HypertensivesDocument23 pagesAnti HypertensivesLeena AlateeqNo ratings yet
- Pharmacology (New)Document42 pagesPharmacology (New)srijelita marbunNo ratings yet
- Tatalaksana Krisis HipertensiDocument38 pagesTatalaksana Krisis HipertensiDr Edi HidayatNo ratings yet
- Emergency DrugDocument264 pagesEmergency Drugasma barhoom100% (1)
- ACLS DrugsDocument16 pagesACLS Drugstostc100% (2)
- Advanced Cardiac Life Support (ACLS) : Novita Sari I1A007066Document58 pagesAdvanced Cardiac Life Support (ACLS) : Novita Sari I1A007066R'punzel CurlyNo ratings yet
- Acls AtpDocument44 pagesAcls AtpDeborah Anasthasia PakpahanNo ratings yet
- Emergency Internal Medicine: Rizal HafizDocument104 pagesEmergency Internal Medicine: Rizal HafizMotivation VoiceNo ratings yet
- On Emergency DrugsDocument25 pagesOn Emergency DrugsBikram Chhetry100% (1)
- MedicationsDocument30 pagesMedicationsvamshidhNo ratings yet
- Management of Shock: Role of Inotropic & Vasoactive DrugsDocument50 pagesManagement of Shock: Role of Inotropic & Vasoactive DrugsbajaocNo ratings yet
- Antihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarDocument52 pagesAntihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarASHUTOSH KHADANGANo ratings yet
- Antihypertensive Drugs.Document35 pagesAntihypertensive Drugs.Abdul WahabNo ratings yet
- Prehospital MedicationsDocument123 pagesPrehospital Medicationshilwaalfi100% (1)
- Case Study NCM 118Document14 pagesCase Study NCM 118Romzy BasañesNo ratings yet
- Biologic CrisisDocument19 pagesBiologic CrisisKharene LirazanNo ratings yet
- Vasoactive TherapyDocument26 pagesVasoactive Therapylidya agustinNo ratings yet
- Vasoactive TherapyDocument26 pagesVasoactive Therapylidya agustin100% (1)
- Pharmacology of Vasopressors and InotropesDocument56 pagesPharmacology of Vasopressors and InotropesBalemlay HailuNo ratings yet
- Emergency Drug (Finale)Document49 pagesEmergency Drug (Finale)SN. CaR67% (3)
- Hypertensive Emergency, El - ShahawyDocument41 pagesHypertensive Emergency, El - ShahawysalwaNo ratings yet
- 6.cardiovascular Supporting DrugsDocument46 pages6.cardiovascular Supporting DrugspraditaNo ratings yet
- Drug Study CARDIODocument17 pagesDrug Study CARDIODiannetotz Morales100% (1)
- Aritmia Dan Kardiotonik Eng UciDocument36 pagesAritmia Dan Kardiotonik Eng UciUci RamadhantyNo ratings yet
- Adr Enaline (Epinephrine) 1mg/ml (1:1000) : Paediatric Cardiac Arrest AlgorhytmDocument13 pagesAdr Enaline (Epinephrine) 1mg/ml (1:1000) : Paediatric Cardiac Arrest AlgorhytmwawaNo ratings yet
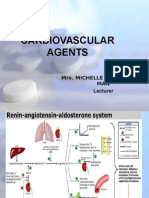
- Cardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerDocument131 pagesCardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerNiala AlmarioNo ratings yet
- Inotropes + Electrolyte Imbalance: Presented By: Asya AmeenDocument53 pagesInotropes + Electrolyte Imbalance: Presented By: Asya AmeenAsia AmeenNo ratings yet
- Antianginal DrugsDocument19 pagesAntianginal DrugsAnusha ZubairNo ratings yet
- Case 02 Arrhythmias 2Document23 pagesCase 02 Arrhythmias 2pqp7mpk7v6No ratings yet
- Obat-Obatan ResusitasiDocument21 pagesObat-Obatan ResusitasiCut Thalya Alissya RahmaNo ratings yet
- Arrythmic DrugsDocument43 pagesArrythmic DrugsjanakaNo ratings yet
- Cardiac Medications:: What's With The Mixing & Matching?Document97 pagesCardiac Medications:: What's With The Mixing & Matching?TinaHoNo ratings yet
- Cardiac Medications: 1. Antiplatelet Aggregation Therapy: Antiplatelet Aggregation TherapyDocument14 pagesCardiac Medications: 1. Antiplatelet Aggregation Therapy: Antiplatelet Aggregation TherapyMaria OnofreiNo ratings yet
- ACLS MedicationsDocument31 pagesACLS MedicationsDrNorNo ratings yet
- AdenosineDocument2 pagesAdenosinejdmedicNo ratings yet
- Chapter 11 Antihypertensive AgentsDocument11 pagesChapter 11 Antihypertensive AgentsChristine Annmarie TapawanNo ratings yet
- Obat Obat EmergencyDocument34 pagesObat Obat EmergencyandyxifNo ratings yet
- Emergency Drugs: Vasoppressors - Recommended by AHADocument4 pagesEmergency Drugs: Vasoppressors - Recommended by AHAJaffy EspirituNo ratings yet
- Acls Drug OverviewDocument2 pagesAcls Drug OverviewShannon Davis100% (1)
- Vasoactive Drugs (PICUCOURSE)Document52 pagesVasoactive Drugs (PICUCOURSE)surasuarezlopezNo ratings yet
- Pharmacology of Anti Hypertensive Agents (For BPT Students)Document17 pagesPharmacology of Anti Hypertensive Agents (For BPT Students)Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Anoosha Roll#21Document19 pagesAnoosha Roll#21Anusha ZubairNo ratings yet
- DRUGS PediatricsDocument42 pagesDRUGS PediatricsRAJ BADMERANo ratings yet
- Obat-Obatan Dalam Bantuan Hidup LanjutDocument16 pagesObat-Obatan Dalam Bantuan Hidup LanjutTheresia SihotangNo ratings yet
- عرض تقديمي2Document18 pagesعرض تقديمي2Sabrina ShalhoutNo ratings yet
- Architecture +design INDIA Feb 2024Document100 pagesArchitecture +design INDIA Feb 2024VENKATESH RAMSALINo ratings yet
- Business Sphere INDIA Feb.2024Document68 pagesBusiness Sphere INDIA Feb.2024VENKATESH RAMSALINo ratings yet
- Absolutely Education Prep and PrePrep-Autumn 2023Document102 pagesAbsolutely Education Prep and PrePrep-Autumn 2023VENKATESH RAMSALINo ratings yet
- Detailed Advertisement Dba and Ddba 22 Sep 2023 21 21Document6 pagesDetailed Advertisement Dba and Ddba 22 Sep 2023 21 21VENKATESH RAMSALINo ratings yet
- 15 - CCLS - PharmacologyDocument32 pages15 - CCLS - PharmacologyVENKATESH RAMSALINo ratings yet
- Inspiron 16 2-In-1 Laptop - Dell USADocument1 pageInspiron 16 2-In-1 Laptop - Dell USAVENKATESH RAMSALINo ratings yet
- Delhi CityDocument4 pagesDelhi CityVENKATESH RAMSALINo ratings yet
- Acute Non Traumatic WeaknessDocument15 pagesAcute Non Traumatic WeaknessVENKATESH RAMSALINo ratings yet
- Business GuardianDocument8 pagesBusiness GuardianVENKATESH RAMSALINo ratings yet
- PuzzlesDocument4 pagesPuzzlesVENKATESH RAMSALINo ratings yet
- Mumbai CityDocument4 pagesMumbai CityVENKATESH RAMSALINo ratings yet
- Senior HGP Module 4 For PrintingDocument23 pagesSenior HGP Module 4 For PrintingEric SapioNo ratings yet
- Sulit 25 3472/1: Kebarangkalian Hujung Atas Q (Z) Bagi Taburan Normal N (0, 1)Document1 pageSulit 25 3472/1: Kebarangkalian Hujung Atas Q (Z) Bagi Taburan Normal N (0, 1)IdalesNo ratings yet
- Exploring Pop Up Libraries in PracticeDocument12 pagesExploring Pop Up Libraries in Practicewilliam_V_LeeNo ratings yet
- Lists of Irrational ThoughtDocument4 pagesLists of Irrational ThoughtJovena Lim0% (1)
- Rconfess eDocument63 pagesRconfess eansar868No ratings yet
- Resume 2Document1 pageResume 2api-375513943No ratings yet
- United States v. Milton Efrain Cruz-Flores, 56 F.3d 461, 2d Cir. (1995)Document4 pagesUnited States v. Milton Efrain Cruz-Flores, 56 F.3d 461, 2d Cir. (1995)Scribd Government DocsNo ratings yet
- Horeca Event by PmiDocument33 pagesHoreca Event by PmiXico ShazzadNo ratings yet
- The Terminal Reaction PaperDocument1 pageThe Terminal Reaction PaperEdward Jayson Santillan100% (1)
- Day 9 What Makes God SmileDocument3 pagesDay 9 What Makes God SmileOktavianus RebitNo ratings yet
- RPA Uipath Multiple Choice Q & ADocument15 pagesRPA Uipath Multiple Choice Q & ABashadada Khadar57% (23)
- Activity-5a ComposingacademicwritingDocument14 pagesActivity-5a ComposingacademicwritingGerold LaderasNo ratings yet
- Sentence Correction Questions FormatDocument6 pagesSentence Correction Questions FormatQamar AbbasNo ratings yet
- Jewish Standard, April 28, 2018Document60 pagesJewish Standard, April 28, 2018New Jersey Jewish Standard100% (1)
- Balance Sheet: 1.total AssetsDocument27 pagesBalance Sheet: 1.total AssetsAmit SharmaNo ratings yet
- Earths Landforms Lesson2Document6 pagesEarths Landforms Lesson2api-242127878No ratings yet
- Homework 7: Right Linear Grammars & CFGS: Due: Nov. 5ThDocument2 pagesHomework 7: Right Linear Grammars & CFGS: Due: Nov. 5ThAndrew ChenNo ratings yet
- Exp 7Document3 pagesExp 7Simi JainNo ratings yet
- READING COMPREHENSION TEST 8vo Básico 24 de MayoDocument1 pageREADING COMPREHENSION TEST 8vo Básico 24 de MayoLeo Sniper WolfNo ratings yet
- Urodynamic Testing ReportDocument25 pagesUrodynamic Testing Reportzharah180% (1)
- The Effects of Digital StorytellingDocument12 pagesThe Effects of Digital StorytellingGuna SegarNo ratings yet
- Book Review: Physics of Radiology, 2nd Ed. by Anthony Brinton Wolbarst. Madison, WI: Medical Physics PublishingDocument1 pageBook Review: Physics of Radiology, 2nd Ed. by Anthony Brinton Wolbarst. Madison, WI: Medical Physics PublishingRoric ThomasNo ratings yet
- Chapter 13Document21 pagesChapter 13Bo ZydarinNo ratings yet
- Written ReportDocument8 pagesWritten ReportMaika VillegasNo ratings yet