You might also like
- Achilies Tendon RepairDocument16 pagesAchilies Tendon Repairapi-611889946No ratings yet
- Take+Care Publication WebDocument83 pagesTake+Care Publication WebSans FictionNo ratings yet
- Pediatric Mechanical VentilationDocument36 pagesPediatric Mechanical VentilationrizalNo ratings yet
- The Shoulder and Shoulder GirdleDocument43 pagesThe Shoulder and Shoulder GirdleMuhammad UsmanNo ratings yet
- Acl Rupturer - TextbookDocument26 pagesAcl Rupturer - TextbookFakhrun Nisa WitringNo ratings yet
- ACE Personal Trainer Manual Chapter 15Document42 pagesACE Personal Trainer Manual Chapter 15Đạt NguyễnNo ratings yet
- Kanski S Clinical Ophthalmology A Systematic.20Document1 pageKanski S Clinical Ophthalmology A Systematic.20dyiah ayuNo ratings yet
- Angela Hand and Upper ExtremityDocument59 pagesAngela Hand and Upper ExtremityJenny RajanNo ratings yet
- Physical Therapy For Sports Injuries (2012-2013)Document66 pagesPhysical Therapy For Sports Injuries (2012-2013)Mohammad EsmatNo ratings yet
- Chronic Shoulder PainDocument28 pagesChronic Shoulder PainThermalBathsforActivNo ratings yet
- Chapter 11 - Injuries - The Hip, Thigh, and PelvisDocument13 pagesChapter 11 - Injuries - The Hip, Thigh, and PelvisSurgicalgownNo ratings yet
- ICF Codes:: Related To The Reported Activity Limitation or Participation RestrictionsDocument19 pagesICF Codes:: Related To The Reported Activity Limitation or Participation RestrictionsHONGJYNo ratings yet
- Stroke (Cerebrovascular Accident) : 1. QXCI Treatment PossibilitiesDocument5 pagesStroke (Cerebrovascular Accident) : 1. QXCI Treatment PossibilitiesEnrique Gonzalez Marquier100% (1)
- Principle of Fracture & Dislocation ManagementDocument118 pagesPrinciple of Fracture & Dislocation ManagementBryan LeongNo ratings yet
- Passivce Range of Motion ExercisesDocument29 pagesPassivce Range of Motion Exercisesvidyasagar pagilla100% (1)
- Case Present AclDocument60 pagesCase Present AclNovell VeliaNo ratings yet
- Slide Kuliah Transfusi DarahDocument31 pagesSlide Kuliah Transfusi Darahfenti nurul khafifahNo ratings yet
- Orthopaedic Emergencies AndreDocument49 pagesOrthopaedic Emergencies AndreLusi MunawarohNo ratings yet
- Nursing Care of The High Risk Newborn To Maturity: Nursing Diagnosis Outcome Evaluation Assessment InterventionDocument9 pagesNursing Care of The High Risk Newborn To Maturity: Nursing Diagnosis Outcome Evaluation Assessment InterventionNur Sanaani100% (1)
- Nasa Pemf Slisci 12Document2 pagesNasa Pemf Slisci 12Homers SimpsonNo ratings yet
- Low Back Pain SlidesDocument27 pagesLow Back Pain SlidesAviv Aziz Triono100% (1)
- Orthopedic Department Medical Faculty Moslem University of IndonesiaDocument14 pagesOrthopedic Department Medical Faculty Moslem University of IndonesiaYunhi SapanNo ratings yet
- PateelaectomyDocument33 pagesPateelaectomybajajmetals08No ratings yet
- Muscle: Assessed Through Dynamometry, Manual Muscle Strength and Functional StrengthDocument12 pagesMuscle: Assessed Through Dynamometry, Manual Muscle Strength and Functional StrengthArifa ShehzadiNo ratings yet
- Group 1 Tutorial IcaDocument7 pagesGroup 1 Tutorial Icaapi-468093714No ratings yet
- 4 5800869459467963727 PDFDocument38 pages4 5800869459467963727 PDFاحمدNo ratings yet
- Daftar Tilik APNDocument17 pagesDaftar Tilik APNmarindadaNo ratings yet
- Restoring Rangeof Motionand Improving FlexibilityDocument35 pagesRestoring Rangeof Motionand Improving FlexibilitysharenNo ratings yet
- Hip Impingement and Labral Tear Non-operative Rehab Protocol-SLU - نسخة PDFDocument2 pagesHip Impingement and Labral Tear Non-operative Rehab Protocol-SLU - نسخة PDFمركز ريلاكس للعلاج الطبيعيNo ratings yet
- Rehabilitation Protocol For Medial Lateral EpicondylitisDocument3 pagesRehabilitation Protocol For Medial Lateral EpicondylitisSantiago BianchiNo ratings yet
- 31hand FlexorTendonRepairDocument3 pages31hand FlexorTendonRepairshera firanaNo ratings yet
- نسخة light blue creative modern medical clinic presentationDocument33 pagesنسخة light blue creative modern medical clinic presentationFaresNo ratings yet
- Management of Elbow Common Injuries: Functional Anatomy Mechanics Epicondylitis Post Immobilization Capsular TightnessDocument31 pagesManagement of Elbow Common Injuries: Functional Anatomy Mechanics Epicondylitis Post Immobilization Capsular TightnessAmany Abd ELfatah HassanNo ratings yet
- ACL Reconstruction RehabilitationDocument12 pagesACL Reconstruction Rehabilitation楊畯凱No ratings yet
- HSSRehabilitationClinicalGuidelines Knee MedialCollateralLigament MCL Sprain Non OperativeDocument12 pagesHSSRehabilitationClinicalGuidelines Knee MedialCollateralLigament MCL Sprain Non OperativeJo CacerNo ratings yet
- Qindeel Fatima Ankle Sprain TreatmentDocument19 pagesQindeel Fatima Ankle Sprain TreatmentQindeel FatimaNo ratings yet
- Total Knee Replacement: Guided By: Dr. Kratika Varshney P.TDocument66 pagesTotal Knee Replacement: Guided By: Dr. Kratika Varshney P.THarshita SharmaNo ratings yet
- Massgeneral Rehabilitation Protocol ACLDocument8 pagesMassgeneral Rehabilitation Protocol ACLcbh94455ycNo ratings yet
- Aclr Protocol JoscDocument9 pagesAclr Protocol JoscJogja Orthopaedic Sport ClinicNo ratings yet
- Group Fitness Instructor University Curriculum: Chapter 8: The Prevention and Management of Common InjuriesDocument34 pagesGroup Fitness Instructor University Curriculum: Chapter 8: The Prevention and Management of Common InjuriesLouis TrầnNo ratings yet
- Introduction To Sports InjuriesDocument31 pagesIntroduction To Sports Injuriesمحمد عقلNo ratings yet
- Total Knee Replacement (TKR) : Dr. Aamer NaeemDocument41 pagesTotal Knee Replacement (TKR) : Dr. Aamer NaeemfaizasaleemsameNo ratings yet
- FlexibilityDocument17 pagesFlexibilityallytubishaNo ratings yet
- 5a4 PCLDocument6 pages5a4 PCLNyemas reda LedistiaNo ratings yet
- Module 3 - THXDocument13 pagesModule 3 - THXZgama AbdulrahmanNo ratings yet
- Rehabilitation Guidelines For Posterior Cruciate Ligament ReconstructionDocument6 pagesRehabilitation Guidelines For Posterior Cruciate Ligament ReconstructionMono MostafaNo ratings yet
- Posterolateral Rotatory Instability of The ElbowDocument16 pagesPosterolateral Rotatory Instability of The ElbowsophiaNo ratings yet
- Groin InjuryDocument17 pagesGroin Injurymateh ur rehmanNo ratings yet
- Soft Tissue Injuries 20208261938130Document41 pagesSoft Tissue Injuries 20208261938130Kavya MittalNo ratings yet
- Epicondylitis Repair - Rehab ProtocolDocument2 pagesEpicondylitis Repair - Rehab ProtocolKiara BrownNo ratings yet
- Total Elbow Arthroplasty and RehabilitationDocument5 pagesTotal Elbow Arthroplasty and RehabilitationMarina ENo ratings yet
- CECS ProtocolDocument6 pagesCECS ProtocolTsz Kwan CheungNo ratings yet
- Acute Injuries of Hip Pelvis and ThighDocument38 pagesAcute Injuries of Hip Pelvis and ThighShrouq BadrNo ratings yet
- Spinal Cord Injury: Andi IhwanDocument31 pagesSpinal Cord Injury: Andi IhwanAndi Muliana SultaniNo ratings yet
- PT Guidelines For Ankle SprainDocument5 pagesPT Guidelines For Ankle SprainKirti GunjikarNo ratings yet
- Taping and Bandaging ReportDocument7 pagesTaping and Bandaging ReportA.M.A AlshehriNo ratings yet
- Anterior GH DislocationDocument6 pagesAnterior GH DislocationDewi HanaNo ratings yet
- Rehab AclDocument71 pagesRehab AclQuang TranNo ratings yet
- Acl RehabilitationDocument40 pagesAcl RehabilitationbrijeshNo ratings yet
- Varieties of Spondylolisthesis: (A) Normal, (B) Congenital, (C) Isthmic, (D) Traumatic, (E) Degenerative, and (F) PathologicalDocument5 pagesVarieties of Spondylolisthesis: (A) Normal, (B) Congenital, (C) Isthmic, (D) Traumatic, (E) Degenerative, and (F) PathologicalYashaswi ANo ratings yet
- PoliomyelitisDocument43 pagesPoliomyelitisGurpreet KaurNo ratings yet
- Chapter 21: The Thigh, Hip, Groin, and PelvisDocument50 pagesChapter 21: The Thigh, Hip, Groin, and PelvisAditya MuchayatsyahNo ratings yet
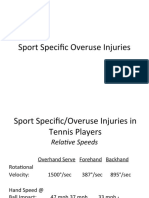
- 2CCSP - Overuse InjuriesDocument70 pages2CCSP - Overuse InjuriesCorey FinanNo ratings yet
- Rehabilitation Guidelines Following Compartment Syndrome Release With Open FasciotomyDocument10 pagesRehabilitation Guidelines Following Compartment Syndrome Release With Open FasciotomyFaridatul IsniyahNo ratings yet
- CH 54: Musculoskeletal Trauma (Per Amendolair)Document54 pagesCH 54: Musculoskeletal Trauma (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- Anterior Cruciate Ligament InjuriesDocument16 pagesAnterior Cruciate Ligament InjuriesAlmas PrawotoNo ratings yet
- Injuri & Trauma Saat Olahraga & Penatalaksanaannya (DR - Arief Faisal, SP - OT)Document53 pagesInjuri & Trauma Saat Olahraga & Penatalaksanaannya (DR - Arief Faisal, SP - OT)Wulan Nindira WarasudiNo ratings yet
- 10 1056@NEJMoa1909406Document11 pages10 1056@NEJMoa1909406alvaroNo ratings yet
- Medical Pro Form ADocument8 pagesMedical Pro Form ASamar SinghNo ratings yet
- The Polyanalgesic Consensus Conference PACC Recommendations For Trialing of Intrathecal Drug Delivery Infusion Therapy. Neuromodulation 2017Document22 pagesThe Polyanalgesic Consensus Conference PACC Recommendations For Trialing of Intrathecal Drug Delivery Infusion Therapy. Neuromodulation 2017Michael HuntNo ratings yet
- Pharmacology Reviewer: Chapter 27: General and Local Anesthetic AgentsDocument10 pagesPharmacology Reviewer: Chapter 27: General and Local Anesthetic AgentsKyla CastroNo ratings yet
- Key and ExplanationDocument4 pagesKey and ExplanationAmelia PhNo ratings yet
- PHARM CARE PD SLE NewDocument58 pagesPHARM CARE PD SLE NewbrevmanaNo ratings yet
- Bone Marrow BiopsyDocument2 pagesBone Marrow BiopsySatinder SinghNo ratings yet
- Analisis Di BukittinggiDocument16 pagesAnalisis Di BukittinggiRachel VictorianaNo ratings yet
- Hodgkin Disease: - DefinitionDocument11 pagesHodgkin Disease: - DefinitionAnurag SharmaNo ratings yet
- Fibromyalgia & Chronic FatigueDocument4 pagesFibromyalgia & Chronic FatigueKarl JacobsNo ratings yet
- Poisoning Drug Overdose 7Th Edition Kent R Olson Ed All ChapterDocument67 pagesPoisoning Drug Overdose 7Th Edition Kent R Olson Ed All Chapterjamison.dean476100% (9)
- Frequencies For FSMDocument5 pagesFrequencies For FSMtd5xb7w4dpNo ratings yet
- Metabolism Clinical and Experimental: Anatoli Petridou, Aikaterina Siopi, Vassilis MougiosDocument7 pagesMetabolism Clinical and Experimental: Anatoli Petridou, Aikaterina Siopi, Vassilis MougiosUjian LancarNo ratings yet
- AttachmentDocument39 pagesAttachmentshmlniz100% (1)
- Vap AssignmentDocument36 pagesVap AssignmentmochkurniawanNo ratings yet
- Medonic m20 Blood Cell CounterDocument129 pagesMedonic m20 Blood Cell Counterроман жуковNo ratings yet
- 9515-184-51-ENG - REV - B1 HScribe Clinicians Guide V5 - 01Document48 pages9515-184-51-ENG - REV - B1 HScribe Clinicians Guide V5 - 01Rodrigo GutierrezNo ratings yet
- BING VITAL SIGN KEL 7-DikonversiDocument2 pagesBING VITAL SIGN KEL 7-DikonversiElvin Elsa MaharennyNo ratings yet
- Laporan-Laporan ObatDocument83 pagesLaporan-Laporan Obatsofyan hadyNo ratings yet
- Jessica Brooks - Resume Nurs 419 1Document1 pageJessica Brooks - Resume Nurs 419 1api-469609100No ratings yet
- Sbar PDFDocument165 pagesSbar PDFseptyNo ratings yet
- Simplifying Active Inhibition TechiquesDocument3 pagesSimplifying Active Inhibition Techiqueseashoor100% (4)