You might also like
- CPAC SON HA 7 Thorax 1Document59 pagesCPAC SON HA 7 Thorax 1misshalieediiNo ratings yet
- 45 Mins or Less to Memorize, Pronounce and Understand Medical Terms. The Best and Most Effective Way to Build Your Medical Vocabulary Quickly!From Everand45 Mins or Less to Memorize, Pronounce and Understand Medical Terms. The Best and Most Effective Way to Build Your Medical Vocabulary Quickly!Rating: 2 out of 5 stars2/5 (2)
- Assessing The Thorax and LungsDocument4 pagesAssessing The Thorax and LungsLorenz Jude Cańete100% (2)
- Review NotesDocument5 pagesReview NotesIrish May BalanzaNo ratings yet
- Assessing The Thorax and Lung PDFDocument9 pagesAssessing The Thorax and Lung PDFYudi TrigunaNo ratings yet
- Physical Examination 2011Document171 pagesPhysical Examination 2011Norakmal Andika YusriNo ratings yet
- The Thorax and Lungs Assessment (Autosaved)Document49 pagesThe Thorax and Lungs Assessment (Autosaved)Arlyn Mendenilla67% (3)
- Cardiovascular (CVS) Examination: Procedure StepsDocument15 pagesCardiovascular (CVS) Examination: Procedure StepsGeorich NarcisoNo ratings yet
- The Thorax and Lungs Assessment (Autosaved)Document49 pagesThe Thorax and Lungs Assessment (Autosaved)Arlyn Mendenilla100% (4)
- Plan:: Around The Circumference of The ChestDocument9 pagesPlan:: Around The Circumference of The ChestPrashant SinghNo ratings yet
- The Thorax and The Lungs: Group 11 FMPDocument27 pagesThe Thorax and The Lungs: Group 11 FMPTisha TancongcoNo ratings yet
- NTILS GuideDocument11 pagesNTILS GuideNeil ThomasNo ratings yet
- Newborn AssessmentDocument17 pagesNewborn Assessmentmarycris100% (2)
- Physical Examination of The Respiratory SystemDocument11 pagesPhysical Examination of The Respiratory SystemMark CatabijanNo ratings yet
- AssesssingDocument20 pagesAssesssingKRISTIAN DRAZEN MIRANDANo ratings yet
- Respiratory Examination GuideDocument4 pagesRespiratory Examination Guiderhea100% (2)
- CASE REPORT - Rheumatoid ArthritisDocument13 pagesCASE REPORT - Rheumatoid ArthritisbrightagbotuiNo ratings yet
- Thorax Breast and Lymphatic System AssesmentDocument106 pagesThorax Breast and Lymphatic System AssesmentJanelle LasalaNo ratings yet
- Assessing The Thorax and The LungsDocument9 pagesAssessing The Thorax and The LungsChrizzia Del RosarioNo ratings yet
- Assessing The Thorax and The LungsDocument9 pagesAssessing The Thorax and The LungsChrizzia Del RosarioNo ratings yet
- Pemeriksaan Abdomen: Dr. Suhaemi, SPPD, FinasimDocument179 pagesPemeriksaan Abdomen: Dr. Suhaemi, SPPD, FinasimiroelnafialyskaNo ratings yet
- De Veyra Assignment WK 3Document12 pagesDe Veyra Assignment WK 3adrian lozanoNo ratings yet
- Pediatric Clinical ExaminationDocument37 pagesPediatric Clinical ExaminationHalema Al OkshNo ratings yet
- A CASE PRESENTATION ON BaiaeDocument35 pagesA CASE PRESENTATION ON Baiaebear_pandaNo ratings yet
- AGN 3B FinalDocument37 pagesAGN 3B FinalKristine Dela CruzNo ratings yet
- 3Q Las Health9 PDFDocument12 pages3Q Las Health9 PDFJairus AbasoloNo ratings yet
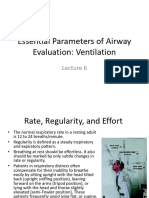
- Essential Parameters of Airway Evaluation Lecture 6Document27 pagesEssential Parameters of Airway Evaluation Lecture 69yqgmkvyzdNo ratings yet
- Week 4 Case 4 Chir13009Document9 pagesWeek 4 Case 4 Chir13009api-479754549No ratings yet
- Physical Examination by DRDocument25 pagesPhysical Examination by DRapi-3739910100% (2)
- Physical ExaminationDocument32 pagesPhysical ExaminationCaroline AgathaNo ratings yet
- New Born AssessmentDocument42 pagesNew Born AssessmentBhawna Joshi100% (3)
- Respiratory AssessmentDocument43 pagesRespiratory AssessmentLui Andrei AnilaNo ratings yet
- DRR LessonsDocument8 pagesDRR LessonsKristel Joy BelgicaNo ratings yet
- Assesment of The Newborn Baby-KuliahDocument66 pagesAssesment of The Newborn Baby-KuliahDhana AstikaNo ratings yet
- Physical Assessment On AdultsDocument12 pagesPhysical Assessment On AdultsGen-GenMedranoGirayNo ratings yet
- OSCE Must Knows For All SubjectsDocument8 pagesOSCE Must Knows For All SubjectsPrincess Jeanne Roque GairanodNo ratings yet
- Presented By:: Rheumatic Heart DiseaseDocument43 pagesPresented By:: Rheumatic Heart DiseaseJerssy TomasNo ratings yet
- Physical ExaminationDocument55 pagesPhysical Examinationdakshpanchal26369No ratings yet
- 8.dx and RPDocument20 pages8.dx and RPkimberlynNo ratings yet
- ASSESSING THORAX and LUNGSDocument25 pagesASSESSING THORAX and LUNGSPrincess AñabezaNo ratings yet
- Respiratory Syatem: January 2009Document19 pagesRespiratory Syatem: January 2009Amit Kiran RathNo ratings yet
- Module - 2-Chest and CVS: Pediatrics 2018-2019 Prof. Yusra AR MahmoodDocument3 pagesModule - 2-Chest and CVS: Pediatrics 2018-2019 Prof. Yusra AR MahmoodHeron EgretNo ratings yet
- Lungs and ThoraxDocument2 pagesLungs and ThoraxKiara Ash BeethovenNo ratings yet
- Thorax and The LungsDocument30 pagesThorax and The Lungschifunndo charles100% (1)
- ملزمة تمريض باطني جراحي الترم الثاني2 التميز +الريادةDocument59 pagesملزمة تمريض باطني جراحي الترم الثاني2 التميز +الريادةabdullah almatary100% (1)
- CP3 Respiratory SystemDocument23 pagesCP3 Respiratory SystemirynNo ratings yet
- Pediatric Assessment TriangleDocument31 pagesPediatric Assessment TriangleblairNo ratings yet
- Pediatric Community Acquired Pneumonia (Pecap) : Case StudyDocument32 pagesPediatric Community Acquired Pneumonia (Pecap) : Case StudyR Hornilla ArcegaNo ratings yet
- Respiratory Syatem: January 2009Document19 pagesRespiratory Syatem: January 2009aarti devNo ratings yet
- Lungs and ThoracicDocument66 pagesLungs and ThoracicJoyce Jacobe0% (1)
- Thoracic and Lung Assessment: Physical Examination of The Thorax and The LungsDocument16 pagesThoracic and Lung Assessment: Physical Examination of The Thorax and The Lungsshannon c. lewis100% (1)
- Postpartum Physical AssessmentDocument60 pagesPostpartum Physical AssessmentAngelica del Mundo88% (8)
- Physical DiagnosisDocument97 pagesPhysical Diagnosisaxmedfare138No ratings yet
- Obstetric Physical ExaminationDocument2 pagesObstetric Physical ExaminationNor Atikah EnddyNo ratings yet
- Abdominal ExaminationDocument180 pagesAbdominal ExaminationAdityaHudiansyah100% (2)
- CAP Case StudyDocument18 pagesCAP Case StudyFlorence Roselle AdalinNo ratings yet
- PE of Neck - NZ FixDocument39 pagesPE of Neck - NZ FixratkhiaberNo ratings yet
- ANSWER KEY-RESPIRATORY Assessment and ReasoningDocument9 pagesANSWER KEY-RESPIRATORY Assessment and ReasoningMaryAnn Tiburcio CuevasNo ratings yet
- Six Components Necessary For Effective Public Health Program ImplementationDocument6 pagesSix Components Necessary For Effective Public Health Program Implementationapi-528624617No ratings yet
- Literature Review On MDR-TBDocument5 pagesLiterature Review On MDR-TBafmzslnxmqrjom100% (1)
- Week 1&2 - CPHM PDFDocument3 pagesWeek 1&2 - CPHM PDFAziz AyobNo ratings yet
- КРОК-1 (microbiology 2009-2020) -перетвореноDocument57 pagesКРОК-1 (microbiology 2009-2020) -перетвореноMA1910o nii odoi patterson100% (1)
- Indigenous Traditional MedicineDocument12 pagesIndigenous Traditional MedicinerathiasNo ratings yet
- CivilsTap - CSAT - English 12Document22 pagesCivilsTap - CSAT - English 12PPPNo ratings yet
- PB 1 - NP 1 (Final)Document19 pagesPB 1 - NP 1 (Final)AnnizaNo ratings yet
- Kamus Indonesia InggrisDocument22 pagesKamus Indonesia InggrisUj ConaruNo ratings yet
- HSM207-Assessment Brief (Update)Document4 pagesHSM207-Assessment Brief (Update)Megha Binu AntonyNo ratings yet
- Health10 - q3 - Mod1 - Health Trends, Issues and Concerns at The Global LevelDocument19 pagesHealth10 - q3 - Mod1 - Health Trends, Issues and Concerns at The Global LevelMark GutangNo ratings yet
- MCQ QuestionsDocument9 pagesMCQ Questionshajra0325No ratings yet
- Soal RespiDocument9 pagesSoal RespiHaidir ArmansyahNo ratings yet
- Tuberculosis Prevention Plan: Histology LaboratoryDocument10 pagesTuberculosis Prevention Plan: Histology LaboratoryLynel Joy JamotilloNo ratings yet
- Aily Equirements: Case: Patient With Tuberculosis General Objectives (5pts)Document31 pagesAily Equirements: Case: Patient With Tuberculosis General Objectives (5pts)janna mae patriarcaNo ratings yet
- Vong 1Document10 pagesVong 1BlissKedNo ratings yet
- Tuberculosis Lecture 1Document34 pagesTuberculosis Lecture 1Samson SeiduNo ratings yet
- Tuberculosis UNIVALLEDocument33 pagesTuberculosis UNIVALLEPaz VidaNo ratings yet
- Mock Board 1Document16 pagesMock Board 1russeldabon24No ratings yet
- Supplementary Readings On Research Undertaking1Document82 pagesSupplementary Readings On Research Undertaking1Henok T Esperanza100% (1)
- Who FCH Cah 00.1Document175 pagesWho FCH Cah 00.1Regita AyuNo ratings yet
- Mcu Form Malaysian Student UgpgDocument12 pagesMcu Form Malaysian Student UgpgzakariaNo ratings yet
- "TB: Silent Killer" Video Assignment Due Tuesday, October 3Document2 pages"TB: Silent Killer" Video Assignment Due Tuesday, October 3ctyre34No ratings yet
- Carlito RRLSDocument10 pagesCarlito RRLSCarlito SatsatinNo ratings yet
- SDG 4. HospitalDocument215 pagesSDG 4. HospitalMuki SimonNo ratings yet
- Mod Hiv FinalDocument130 pagesMod Hiv Finalpb infornon100% (1)
- Final ResearchDocument64 pagesFinal Researchhundasa chalaNo ratings yet
- Global Health InitiativesDocument31 pagesGlobal Health InitiativesDaisy Joy SalanNo ratings yet
- 3rd Grading Period PDFDocument93 pages3rd Grading Period PDFJuan DiazNo ratings yet
- General Education: St. Louis Review Center, IncDocument13 pagesGeneral Education: St. Louis Review Center, IncRowell DC TrinidadNo ratings yet
- History: Tuberculosis (TB)Document24 pagesHistory: Tuberculosis (TB)Rashed ShatnawiNo ratings yet