You might also like
- 3 Manacsa&Tan 2012 Strong Republic SidetrackedDocument41 pages3 Manacsa&Tan 2012 Strong Republic SidetrackedGil Osila JaradalNo ratings yet
- Psych 1xx3 Quiz AnswersDocument55 pagesPsych 1xx3 Quiz Answerscutinhawayne100% (4)
- CASE PRES PreeclampsiaDocument51 pagesCASE PRES PreeclampsiaRaiza Love Caparas-PablicoNo ratings yet
- Community HelpersDocument3 pagesCommunity Helpersapi-252790280100% (1)
- MKTG 2126 - Assignment 3Document2 pagesMKTG 2126 - Assignment 3omar mcintoshNo ratings yet
- Aka GMP Audit FormDocument8 pagesAka GMP Audit FormAlpian BosixNo ratings yet
- Viral Hepatitis With Dengue Fever: by Jemy Jose Reg No 16Q3506 IV Pharm .DDocument19 pagesViral Hepatitis With Dengue Fever: by Jemy Jose Reg No 16Q3506 IV Pharm .DJEMY JOSENo ratings yet
- Case Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172Document18 pagesCase Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172AmalinNo ratings yet
- Case Study On Acute Gastroenteritis and Acid Peptic-2Document15 pagesCase Study On Acute Gastroenteritis and Acid Peptic-2FHAMITHANo ratings yet
- BA With UTIDocument20 pagesBA With UTIJyothsna JoyNo ratings yet
- Case Study On: Alcoholic Hepatitis With Jaundice With UtiDocument19 pagesCase Study On: Alcoholic Hepatitis With Jaundice With UtiBhagya KurianNo ratings yet
- Decompensated Liver DiseaseDocument16 pagesDecompensated Liver Diseasedk.clinicalresearchNo ratings yet
- CASE 1 pharmacotherapeuticsDocument14 pagesCASE 1 pharmacotherapeuticsOmair Mohammed 19No ratings yet
- Ald With Acute Gastroenteritis With Portal HTN With PancytopeniaDocument17 pagesAld With Acute Gastroenteritis With Portal HTN With PancytopeniaBhagya KurianNo ratings yet
- Case Presentation ON Accelerated HypertensionDocument30 pagesCase Presentation ON Accelerated HypertensionJigeesha LakshmiNo ratings yet
- Fever with Chills and Rigors: A Case of MalariaDocument19 pagesFever with Chills and Rigors: A Case of MalariaREETHUNo ratings yet
- Stroke by K. NusrithaDocument13 pagesStroke by K. NusrithaSai SharathNo ratings yet
- CASE PRESENTATION ON AnemiaDocument25 pagesCASE PRESENTATION ON AnemiaSafoora Rafeeq100% (2)
- Case Presentation On Chronic BronchitisDocument20 pagesCase Presentation On Chronic BronchitisSafoora RafeeqNo ratings yet
- POMR Satiti Acute CholangitisDocument30 pagesPOMR Satiti Acute CholangitisIka AyuNo ratings yet
- CASE-STUDY-Infectious DiseaseDocument8 pagesCASE-STUDY-Infectious DiseaseJoshua RamirezNo ratings yet
- Bloody vomiting and melena case summariesDocument16 pagesBloody vomiting and melena case summariesmiaNo ratings yet
- Morning ReportDocument27 pagesMorning ReportDody PrasetyaNo ratings yet
- Heaptic EncephalopathyDocument16 pagesHeaptic Encephalopathydk.clinicalresearchNo ratings yet
- Morning Report: Date: 1 June 2019Document15 pagesMorning Report: Date: 1 June 2019Erwin HidayatNo ratings yet
- Patient DemographicsDocument9 pagesPatient DemographicsIzaan Ahmed KhanNo ratings yet
- Case ReportDocument34 pagesCase ReportMiftahul JannahNo ratings yet
- Dengue Fever (A90) + Nosocomial Condition (Y95) : Case ReportDocument22 pagesDengue Fever (A90) + Nosocomial Condition (Y95) : Case ReportMafisahNo ratings yet
- Ibdcase 180706145428 PDFDocument15 pagesIbdcase 180706145428 PDFakashNo ratings yet
- NC - Immanuel Ata TuruDocument20 pagesNC - Immanuel Ata TuruDodi DiNo ratings yet
- Aki C PeDocument16 pagesAki C Pedk.clinicalresearchNo ratings yet
- Presented by Abhishek U N 5 Pharm D 17Q1001: Case Presentation On Alcoholic Liver Disease With HypertensionDocument19 pagesPresented by Abhishek U N 5 Pharm D 17Q1001: Case Presentation On Alcoholic Liver Disease With Hypertensionlast requestNo ratings yet
- DepartmentDocument7 pagesDepartmentmubarek abdurohemanNo ratings yet
- Case Presentation On Parkinson'S Disease: Presented By: T.Avinash Vith Pharm D Y13PHD0721Document21 pagesCase Presentation On Parkinson'S Disease: Presented By: T.Avinash Vith Pharm D Y13PHD0721AVINASH TALAPALA100% (1)
- Case Presentation On Twisted Ovarian Cyst: B Geethavani 13DK1T0002 Pharm D InternDocument19 pagesCase Presentation On Twisted Ovarian Cyst: B Geethavani 13DK1T0002 Pharm D InterngeethaNo ratings yet
- GE BasavaDocument21 pagesGE BasavaAmalin PrãdhãñNo ratings yet
- 91-Year-Old Patient Report with Gastrointestinal BleedingDocument17 pages91-Year-Old Patient Report with Gastrointestinal BleedingPuteri Diah RahtiniNo ratings yet
- Case Presentation On Pres With Seizures: R.G.Nikitha 616175802026 V/VI Pharm. D, Shri Vishnu College of PharmacyDocument17 pagesCase Presentation On Pres With Seizures: R.G.Nikitha 616175802026 V/VI Pharm. D, Shri Vishnu College of Pharmacysrija vijjapuNo ratings yet
- CASE PRESENTATION ON TUBERCULOSISASE - Pavani TekumallaDocument29 pagesCASE PRESENTATION ON TUBERCULOSISASE - Pavani TekumallaJarvisNo ratings yet
- Presentation On UrosepsisDocument20 pagesPresentation On UrosepsisNewtan DebNo ratings yet
- NC - Muh HafizDocument16 pagesNC - Muh HafizDodi DiNo ratings yet
- ALD WITH ASCITES by VaibhavDocument22 pagesALD WITH ASCITES by VaibhavSandeep ChakravarthyNo ratings yet
- OHSS Case Presentation Discussion - Jindal IVF CHDDocument41 pagesOHSS Case Presentation Discussion - Jindal IVF CHDJindal IVF ChandigarhNo ratings yet
- Morning Report: Date: Monday, 2 November 2020Document24 pagesMorning Report: Date: Monday, 2 November 2020Ika AyuNo ratings yet
- Case Presentation On Ischemic StrokeDocument19 pagesCase Presentation On Ischemic StrokeNayak DrNareshNo ratings yet
- Umbilical Hernia With NephrolithiasisDocument17 pagesUmbilical Hernia With Nephrolithiasisdk.clinicalresearchNo ratings yet
- Case PresentationDocument22 pagesCase PresentationManjunath ArunachalamNo ratings yet
- 18.1 Peritonitis TB - Bedah - DR - Regi RInaldy BDocument47 pages18.1 Peritonitis TB - Bedah - DR - Regi RInaldy BDevi Christina Damanik (Papua medical School)No ratings yet
- Morning Report: Dr. Satya Leads Hospital TeamsDocument42 pagesMorning Report: Dr. Satya Leads Hospital TeamsPramudia DeniNo ratings yet
- Acid Peptic Disease Case StudyDocument11 pagesAcid Peptic Disease Case StudyFHAMITHA100% (1)
- Case Study of Patient With CholelithiasisDocument3 pagesCase Study of Patient With CholelithiasisBer AnneNo ratings yet
- Remon CovidDocument13 pagesRemon CovidJuli2022 Semnol-SemsaNo ratings yet
- Morning Report: Monday, 8 May 2017Document25 pagesMorning Report: Monday, 8 May 2017HarisNo ratings yet
- Case Presentation On TIA and IHDDocument14 pagesCase Presentation On TIA and IHDS SAI BALAJI IYERNo ratings yet
- Lapjag 10 Feb 2016 - AnemiaDocument25 pagesLapjag 10 Feb 2016 - AnemiamyoganoNo ratings yet
- Non ST-Elevated Myocardial Infarction with Acute Decompensated Heart FailureDocument40 pagesNon ST-Elevated Myocardial Infarction with Acute Decompensated Heart FailureNissaIsfadinaSNo ratings yet
- Hydronephrosis of Left KidneyDocument40 pagesHydronephrosis of Left KidneyVandana ReddyNo ratings yet
- Lab Parameter DAY-1 Normal Value: 13.7gms% 8900c/cmm 4000-11000c/cmm 4.8m/cmm 4.3-5.7c/mmDocument6 pagesLab Parameter DAY-1 Normal Value: 13.7gms% 8900c/cmm 4000-11000c/cmm 4.8m/cmm 4.3-5.7c/mmSafoora RafeeqNo ratings yet
- Asma, Cap, TBDocument9 pagesAsma, Cap, TByuliaNo ratings yet
- MR DM Hematemesis IMADocument15 pagesMR DM Hematemesis IMANadine BushNo ratings yet
- CASE PRESENTATION ON U AnginaDocument40 pagesCASE PRESENTATION ON U AnginaSafoora RafeeqNo ratings yet
- Macabali GS2Document4 pagesMacabali GS2Christian Edward MacabaliNo ratings yet
- C. Diff Toxin AssayDocument15 pagesC. Diff Toxin AssayMaira KhanNo ratings yet
- HEMIPARESISDocument31 pagesHEMIPARESISMaira KhanNo ratings yet
- MeningitisDocument30 pagesMeningitisMaira KhanNo ratings yet
- HEMIPARESISDocument31 pagesHEMIPARESISMaira KhanNo ratings yet
- LETTER OF AUTHORIZATION CREDO INVEST DownloadDocument1 pageLETTER OF AUTHORIZATION CREDO INVEST DownloadEsteban Enrique Posan BalcazarNo ratings yet
- The Joint Force Commander's Guide To Cyberspace Operations: by Brett T. WilliamsDocument8 pagesThe Joint Force Commander's Guide To Cyberspace Operations: by Brett T. Williamsأريزا لويسNo ratings yet
- Nettoplcsim S7online Documentation en v0.9.1Document5 pagesNettoplcsim S7online Documentation en v0.9.1SyariefNo ratings yet
- Safety Data Sheet: 1. Identification of The Substance/preparation and of The Company/undertakingDocument4 pagesSafety Data Sheet: 1. Identification of The Substance/preparation and of The Company/undertakingBalasubramanian AnanthNo ratings yet
- Unit 7 Noun ClauseDocument101 pagesUnit 7 Noun ClauseMs. Yvonne Campbell0% (1)
- Coffee TestDocument6 pagesCoffee TestAmit Satyen RaviNo ratings yet
- 2023 Catalog Score SummerDocument65 pages2023 Catalog Score Summermadhudasa0% (2)
- TLM4ALL@1 Number System (EM)Document32 pagesTLM4ALL@1 Number System (EM)jkc collegeNo ratings yet
- Satisfaction ExtraDocument2 pagesSatisfaction ExtraFazir AzlanNo ratings yet
- Sato Printer Api Reference DocumentDocument34 pagesSato Printer Api Reference Documentsupersteel.krwNo ratings yet
- Arduino Programming Step by Step Guide To Mastering Arduino Hardware and SoftwareDocument109 pagesArduino Programming Step by Step Guide To Mastering Arduino Hardware and SoftwareMohan100% (3)
- Map Project Rubric 2018Document2 pagesMap Project Rubric 2018api-292774341No ratings yet
- Ncm110nif Midterm Laboratory NotesDocument12 pagesNcm110nif Midterm Laboratory NotesMicah jay MalvasNo ratings yet
- 0520 Int OTG P4 MSDocument12 pages0520 Int OTG P4 MSTrévina JosephNo ratings yet
- AlternatorDocument3 pagesAlternatorVatsal PatelNo ratings yet
- Financial ManagementDocument2 pagesFinancial ManagementSanna KazmiNo ratings yet
- CS6711 Security Lab ManualDocument84 pagesCS6711 Security Lab ManualGanesh KumarNo ratings yet
- Red Lion Edict-97 - Manual PDFDocument282 pagesRed Lion Edict-97 - Manual PDFnaminalatrukNo ratings yet
- Unit 2 Water Treatment Ce3303Document18 pagesUnit 2 Water Treatment Ce3303shivaNo ratings yet
- Covid 19 PDFDocument117 pagesCovid 19 PDFvicky anandNo ratings yet
- Summative Test For Quadratic Equations2Document2 pagesSummative Test For Quadratic Equations2AsmiraMangontra0% (1)
- The Completely Randomized Design (CRD)Document16 pagesThe Completely Randomized Design (CRD)Rahul TripathiNo ratings yet
- Phy Worksheet IG 3 Phase 2Document6 pagesPhy Worksheet IG 3 Phase 2Umair RazaNo ratings yet
- Frequently Asked Questions About Ailunce HD1: Where Can Find HD1 Software & Firmware?Document5 pagesFrequently Asked Questions About Ailunce HD1: Where Can Find HD1 Software & Firmware?Eric Contra Color0% (1)
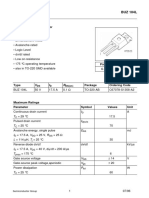
- Sipmos Power Transistor: BUZ 104LDocument10 pagesSipmos Power Transistor: BUZ 104LAlexsander MeloNo ratings yet