You might also like
- Central Theme of ChapterDocument10 pagesCentral Theme of ChapterPrashant PandeyNo ratings yet
- Biaoavaibality & Bioequivalence: F Bioavailable Dose / Administered DoseDocument10 pagesBiaoavaibality & Bioequivalence: F Bioavailable Dose / Administered DoseDipak bariNo ratings yet
- Bioaviabality Bioequivalence 2nd Sem M.pharm PDFDocument10 pagesBioaviabality Bioequivalence 2nd Sem M.pharm PDFDipak bariNo ratings yet
- BioavailabilityDocument35 pagesBioavailabilityDr. Bharat JainNo ratings yet
- Bio Availability and Bio EquivalenceDocument32 pagesBio Availability and Bio Equivalenceكسلان اكتب اسمي100% (1)
- BioavailabilityDocument30 pagesBioavailabilitymuhammadyawarsaeed4No ratings yet
- BIOAVAILABILITY AND BIOEQUIVALENCE STUDIESDocument49 pagesBIOAVAILABILITY AND BIOEQUIVALENCE STUDIESvarishNo ratings yet
- Bioavailability & Bioequivalence ReportDocument19 pagesBioavailability & Bioequivalence ReportKESHAV SINGHNo ratings yet
- Bio Lec.7Document14 pagesBio Lec.7taha.21ph119No ratings yet
- Bioavailability and BioequivalenceDocument23 pagesBioavailability and BioequivalenceSaeed RashidNo ratings yet
- Bioavailability and BioequivalenceDocument81 pagesBioavailability and BioequivalenceNiharika ModiNo ratings yet
- DR Rajesh MujariyaDocument22 pagesDR Rajesh MujariyaRajesh MujariyaNo ratings yet
- BiopharmaceuticsDocument21 pagesBiopharmaceuticsSilvy100% (1)
- Toxicology and Pharmacology GuideDocument41 pagesToxicology and Pharmacology GuideLara GatbontonNo ratings yet
- Pharmacology in Drug Discovery: Understanding Drug ResponseFrom EverandPharmacology in Drug Discovery: Understanding Drug ResponseNo ratings yet
- BIOAVAILABILITY KEY FACTSDocument38 pagesBIOAVAILABILITY KEY FACTSsaadNo ratings yet
- Bahan Kuliah, BioavaibilityDocument26 pagesBahan Kuliah, BioavaibilityMuhammad HilmiNo ratings yet
- Bension Mirzakan - IPPE Assignment 1.13Document4 pagesBension Mirzakan - IPPE Assignment 1.13bmirzakanNo ratings yet
- Bioavailability and BioequivalenceDocument82 pagesBioavailability and Bioequivalenceكسلان اكتب اسمي100% (1)
- 2 Amrutaobjectivesandconsiderationsinbioavailabilitystudy 130211000517 Phpapp01 PDFDocument31 pages2 Amrutaobjectivesandconsiderationsinbioavailabilitystudy 130211000517 Phpapp01 PDFsaurabh chaturvediNo ratings yet
- Introduction to BP-PK & LADMER SystemsDocument26 pagesIntroduction to BP-PK & LADMER SystemsAbdul Mannan80% (5)
- Bioassay Methods for Evaluating DrugsDocument44 pagesBioassay Methods for Evaluating DrugsPrachi Karia100% (7)
- Biopharmaceutics and PharmacokineticsDocument69 pagesBiopharmaceutics and PharmacokineticsRiczen Mae F. Vila100% (1)
- Introduction To Biopharmaceutics and PharmacokineticsDocument29 pagesIntroduction To Biopharmaceutics and PharmacokineticsNasima Begum100% (1)
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- Dose Response StudiesDocument2 pagesDose Response StudiesSooraj Rajasekharan KarthaNo ratings yet
- 1important DefinitionsDocument3 pages1important DefinitionsBest VideoNo ratings yet
- Drug Development and EvaluationDocument25 pagesDrug Development and EvaluationArlises SinagaNo ratings yet
- Sustained Release Drug Delivery System: A Seminar ONDocument109 pagesSustained Release Drug Delivery System: A Seminar ONRajesh KumarNo ratings yet
- Therapeutic Drug Monitoring GuideDocument33 pagesTherapeutic Drug Monitoring GuideDr. Raghavendra Kumar GundaNo ratings yet
- Pharmacokinetics: Pharmacokinetics (In Greek: "Pharmacon" Meaning Drug and "Kinetikos" MeaningDocument5 pagesPharmacokinetics: Pharmacokinetics (In Greek: "Pharmacon" Meaning Drug and "Kinetikos" Meaning0921pyNo ratings yet
- Dr. Ruth NamyaloDocument62 pagesDr. Ruth NamyaloHarun MohamedNo ratings yet
- Therapeutic Drug Monitoring: Saeed Alqahtani, Pharmd, PHDDocument78 pagesTherapeutic Drug Monitoring: Saeed Alqahtani, Pharmd, PHDAnonymous hF5zAdvwCC50% (2)
- Bioavailability of DrugsDocument17 pagesBioavailability of DrugsLodhi MohasinNo ratings yet
- PK & Bioavailability Study of DrugsDocument32 pagesPK & Bioavailability Study of Drugsmursidstone.mursid50% (2)
- BIOASSAYDocument78 pagesBIOASSAYAshly chackoNo ratings yet
- Biopharmaceutics & pharmacokinetics-II AssignmentDocument7 pagesBiopharmaceutics & pharmacokinetics-II AssignmentRA TanvirNo ratings yet
- Review Article Dose-Dependent Pharmacokinetics: Experimental Observations and Theoretical ConsiderationsDocument31 pagesReview Article Dose-Dependent Pharmacokinetics: Experimental Observations and Theoretical Considerationsירדן לויןNo ratings yet
- Toxicokinetics: Sheila SchwartzDocument14 pagesToxicokinetics: Sheila SchwartzVe SeptianaNo ratings yet
- Introduction To PharmacokineticsDocument16 pagesIntroduction To PharmacokineticsMae Quenie Abadingo TiroNo ratings yet
- Bio PharmaceuticsDocument18 pagesBio PharmaceuticsHazel Ruth Yara Castillo100% (1)
- PharmacokineticsDocument10 pagesPharmacokineticsAnkit VermaNo ratings yet
- TherapeuticDocument17 pagesTherapeuticsaad najNo ratings yet
- Therapeutic Drug Monitoring Part 2 PDFDocument23 pagesTherapeutic Drug Monitoring Part 2 PDFChandra AvicennaNo ratings yet
- 1 IntroductionDocument68 pages1 Introductiondona donneNo ratings yet
- Repetition Following Amelioration in Homoeopathy A Randomized Placebo Controlled Pilot StudyDocument7 pagesRepetition Following Amelioration in Homoeopathy A Randomized Placebo Controlled Pilot StudyHomoeopathic PulseNo ratings yet
- Dose-Response ConceptDocument56 pagesDose-Response ConceptAshish GoelNo ratings yet
- Clinical Pharmacokinetics Therapeutic Drug MonitoringDocument41 pagesClinical Pharmacokinetics Therapeutic Drug MonitoringTrifena Prisca MosseNo ratings yet
- Bioavailability - and - Bioequivalence - 2 PDFDocument18 pagesBioavailability - and - Bioequivalence - 2 PDFdilka dariyaNo ratings yet
- Therapeutic Drug Monitoring 7-1-20Document27 pagesTherapeutic Drug Monitoring 7-1-20mofadhilNo ratings yet
- Pharmaco KineticsDocument427 pagesPharmaco KineticsMehrdad AvestaNo ratings yet
- Bioavailability Studies. Chap 3-2Document40 pagesBioavailability Studies. Chap 3-2dilka dariyaNo ratings yet
- Kinetics of Single and Multple Idoses of DrugsDocument46 pagesKinetics of Single and Multple Idoses of DrugsSunilNo ratings yet
- Pharmacology Bioassay GuideDocument27 pagesPharmacology Bioassay GuideAbhijeet MihirNo ratings yet
- Measure Drug ConcentrationsDocument7 pagesMeasure Drug ConcentrationsCarmila Olbe ArroyoNo ratings yet
- Bio Case StudyDocument20 pagesBio Case StudyMd. Nure Alamin SiddikNo ratings yet
- 1-Lecture One IntroductionDocument45 pages1-Lecture One IntroductionKerolus Joseph AminNo ratings yet
- Clinical PharmacologDocument81 pagesClinical PharmacologSHILOTANo ratings yet
- IOM Pharmacology IDocument93 pagesIOM Pharmacology ISahara MahatNo ratings yet
- Rubber Extract1Document11 pagesRubber Extract1anbuchelvanNo ratings yet
- TM 9-2320-340-10Document924 pagesTM 9-2320-340-10Advocate100% (2)
- Structure of Atoms and Symbols of ElementsDocument4 pagesStructure of Atoms and Symbols of ElementsWilrose BarbacionNo ratings yet
- Disclosure To Promote The Right To InformationDocument14 pagesDisclosure To Promote The Right To InformationHafa LabNo ratings yet
- D 877-02 PDFDocument6 pagesD 877-02 PDFAndresNo ratings yet
- O Rings HandbookDocument292 pagesO Rings HandbookleocastarlenasNo ratings yet
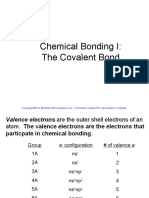
- Chemical Bonding I The Covalent Bond Copyright © The McGraw-Hill CompaniesDocument87 pagesChemical Bonding I The Covalent Bond Copyright © The McGraw-Hill CompaniesRoll OutNo ratings yet
- Everything You Need to Know About Clay Blocks for ConstructionDocument20 pagesEverything You Need to Know About Clay Blocks for ConstructionNidhi MehtaNo ratings yet
- SNG and LPG Systems Overview PDFDocument57 pagesSNG and LPG Systems Overview PDFMohanad100% (1)
- Mechanical Properties of Metals LectureDocument24 pagesMechanical Properties of Metals LectureChuongNo ratings yet
- General Chemistry 1 Activity Sheet Quarter 2-MELC 12 Week 6Document9 pagesGeneral Chemistry 1 Activity Sheet Quarter 2-MELC 12 Week 6Joshua De La VegaNo ratings yet
- Msds Nitrogen DioxideDocument8 pagesMsds Nitrogen DioxideBudiSetiawanNo ratings yet
- SBL1023 Techniques in Biological and Biochemistry LaboratoryDocument5 pagesSBL1023 Techniques in Biological and Biochemistry Laboratoryapi-383715002No ratings yet
- National Technical Regulation On Energy Efficiency BuildingsDocument35 pagesNational Technical Regulation On Energy Efficiency BuildingsTung chu baNo ratings yet
- ClobazamDocument4 pagesClobazamLuwinda SariNo ratings yet
- In Vitro Antibacterial Activity and Phytochemical Profiling of Indonesian Anacardium Occidentale L. Leaf Extract and FractionsDocument23 pagesIn Vitro Antibacterial Activity and Phytochemical Profiling of Indonesian Anacardium Occidentale L. Leaf Extract and FractionsJournal of Pharmacy & Pharmacognosy ResearchNo ratings yet
- Hybrid Anoxic ReactorDocument7 pagesHybrid Anoxic ReactorThirumurugan PandiyanNo ratings yet
- AIGA 074 - 11 Safe Handling of CO2 Containers That Have Lost Pressure - Reformated Jan 12 PDFDocument30 pagesAIGA 074 - 11 Safe Handling of CO2 Containers That Have Lost Pressure - Reformated Jan 12 PDFAnjali Anju100% (1)
- Advanced IC Engines: Prof. R. Devaraj Dr. S. Ramachandran Dr. A. AndersonDocument61 pagesAdvanced IC Engines: Prof. R. Devaraj Dr. S. Ramachandran Dr. A. AndersonGopi KrishnanNo ratings yet
- Introduction to Advanced Manufacturing ProcessesDocument25 pagesIntroduction to Advanced Manufacturing ProcessesAmilin HatiaraNo ratings yet
- Adasil DCSDocument1 pageAdasil DCSMuhammad Aasim HassanNo ratings yet
- Lake and Hirasaki (1981) (SPE-8436-PA)Document10 pagesLake and Hirasaki (1981) (SPE-8436-PA)Anonymous PO7VwbBnNo ratings yet
- Lab Report Vicat TestDocument2 pagesLab Report Vicat TestmanNo ratings yet
- Plastic Roads (Ang)Document17 pagesPlastic Roads (Ang)Feryani DoniaNo ratings yet
- Cement ManufacturingDocument6 pagesCement ManufacturingMuhammad TausifNo ratings yet
- ChE 140 - Sulfur and Sulfuric AcidDocument29 pagesChE 140 - Sulfur and Sulfuric AcidMarialie EnecioNo ratings yet
- Denver Equipment Company Handbook guides engineersDocument0 pagesDenver Equipment Company Handbook guides engineersalvarezri100% (1)
- Chemistry PDFDocument113 pagesChemistry PDFShubham YadavNo ratings yet
- Hydrogen Fuel of The FutureDocument184 pagesHydrogen Fuel of The FutureDefEntNo ratings yet