You might also like
- Clinical Finalterm (9th Sem)Document52 pagesClinical Finalterm (9th Sem)sarwar sonsNo ratings yet
- LaryngitisDocument4 pagesLaryngitisandrewwilliampalileo@yahoocomNo ratings yet
- Understanding TonsillitisDocument2 pagesUnderstanding TonsillitisMarjun JacosalemNo ratings yet
- Respiratory Tract InfectionDocument30 pagesRespiratory Tract InfectionNaresh JoshiNo ratings yet
- Upper Respiratory Tract Infections Group 1 BSN 2.3Document57 pagesUpper Respiratory Tract Infections Group 1 BSN 2.3Joedelynne Diane Endaya GarciaNo ratings yet
- Lesson Notes On UrtiDocument9 pagesLesson Notes On UrtiNeethupaulNo ratings yet
- Respiratory and CirculatoryDocument35 pagesRespiratory and CirculatoryTumabangNo ratings yet
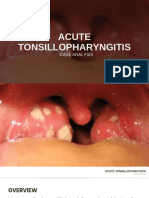
- Acute Tonsillopharyngitis Case AnalysisDocument13 pagesAcute Tonsillopharyngitis Case Analysisrenz bartolomeNo ratings yet
- LARYNGITISDocument5 pagesLARYNGITISNisha CainarNo ratings yet
- Upper Airway InfectionDocument47 pagesUpper Airway Infectionjm_john0% (1)
- Ent Lesson 4Document64 pagesEnt Lesson 4favourednancie9No ratings yet
- Upper Respiratory Tract InfectionsDocument73 pagesUpper Respiratory Tract InfectionsankitaNo ratings yet
- Epiglottitis: Causes, Incidence, and Risk FactorsDocument5 pagesEpiglottitis: Causes, Incidence, and Risk FactorscnvNo ratings yet
- Upper Respiratory Tract InfectionDocument45 pagesUpper Respiratory Tract InfectionNatasha Abdulla100% (2)
- Upper Respiratory Infection (URI/Common Cold) : Kathly M. Jean-Gilles, MSN, RN, RRT-NPS, FNP Gregory A. Wagoner, MD, MBADocument4 pagesUpper Respiratory Infection (URI/Common Cold) : Kathly M. Jean-Gilles, MSN, RN, RRT-NPS, FNP Gregory A. Wagoner, MD, MBAadhiztinenNo ratings yet
- Upper Respiratoty Tract InfectionsDocument10 pagesUpper Respiratoty Tract InfectionsyoshiNo ratings yet
- 1.0 Upper Airway InfectionsDocument45 pages1.0 Upper Airway InfectionsMariahNo ratings yet
- PharyngitisDocument6 pagesPharyngitisJeriel DelavinNo ratings yet
- Report NminDocument7 pagesReport NminGena ManimtimNo ratings yet
- Chapter10 INFLAMMATORY CONDITION OF NOSE & PNSDocument38 pagesChapter10 INFLAMMATORY CONDITION OF NOSE & PNSSULDAANUL CAASHIQIINNo ratings yet
- Respiratory Tract InfectionsDocument42 pagesRespiratory Tract InfectionsRoshana MallawaarachchiNo ratings yet
- Pharygitis AND TonsillitisDocument29 pagesPharygitis AND Tonsillitisstara123No ratings yet
- Clearing The Throat: Coughs Affected PartDocument6 pagesClearing The Throat: Coughs Affected Partkarla callejaNo ratings yet
- Upper RespiratoryDocument51 pagesUpper RespiratoryMelanie D'artistNo ratings yet
- Disorder of ThroatDocument21 pagesDisorder of ThroatSumit YadavNo ratings yet
- Upper Respiratory Tract InfectionDocument43 pagesUpper Respiratory Tract InfectionNaresh JoshiNo ratings yet
- URTIDocument41 pagesURTIGetaneh LiknawNo ratings yet
- Common ColdDocument17 pagesCommon ColdNyakie MotlalaneNo ratings yet
- Disorders of The Respiratory SystemDocument47 pagesDisorders of The Respiratory SystemShweta RamolaNo ratings yet
- Oxygenation ReviewerDocument8 pagesOxygenation ReviewerDamie FernandezNo ratings yet
- Chapter 22 Management of Patients With Upper Respiratory Tract DisordersDocument7 pagesChapter 22 Management of Patients With Upper Respiratory Tract DisordersPeej Reyes100% (2)
- Communicable DiseasesDocument14 pagesCommunicable DiseasesGerald AlNo ratings yet
- When To See Your GP: AntibioticsDocument4 pagesWhen To See Your GP: AntibioticsMounir ChadliNo ratings yet
- Respi SDG Cluster3Document45 pagesRespi SDG Cluster3faye kimNo ratings yet
- What Is TonsillitisDocument3 pagesWhat Is TonsillitisllovemelovemeNo ratings yet
- Common Health Problems of Infancy PowptDocument78 pagesCommon Health Problems of Infancy PowptCiella Dela CruzNo ratings yet
- CN112B (Graded Discussion 3 - Evangelista, Allysa Joi M.)Document3 pagesCN112B (Graded Discussion 3 - Evangelista, Allysa Joi M.)Camille SanguyoNo ratings yet
- Hoarse Voice (Laryngitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHoarse Voice (Laryngitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Revision:: Rhinitis: 1-Acute (Common Cold) 2-Allergic .. Pharyngitis (Sore Throat)Document22 pagesRevision:: Rhinitis: 1-Acute (Common Cold) 2-Allergic .. Pharyngitis (Sore Throat)yuddNo ratings yet
- Sken 3 HoarseDocument9 pagesSken 3 HoarsearyaNo ratings yet
- Botany AssignmentDocument21 pagesBotany Assignmentabdul hadiNo ratings yet
- Coughs & ColdsDocument20 pagesCoughs & Coldsangelstar24087381No ratings yet
- AssignmentDocument8 pagesAssignmentMaria MushtaqueNo ratings yet
- Sore Throat PDFDocument2 pagesSore Throat PDFHappy Martha NababanNo ratings yet
- Acute Viral RhinitisDocument4 pagesAcute Viral RhinitisDebbie beeNo ratings yet
- RESPIRATORYPOWERPOINTDocument81 pagesRESPIRATORYPOWERPOINTarmanuel1390antNo ratings yet
- Acute TonsillitisDocument22 pagesAcute Tonsillitisg0ldz21100% (10)
- LaryngitisDocument2 pagesLaryngitisDian PrimaNo ratings yet
- LaryngitisDocument11 pagesLaryngitisvirendra singhNo ratings yet
- Microbial Infection Respiratory SystemDocument100 pagesMicrobial Infection Respiratory SystemBasty BautistaNo ratings yet
- Respiratory DisordersDocument19 pagesRespiratory DisordersMbalenhleNo ratings yet
- Upper Respiratory Tract InfectionsDocument26 pagesUpper Respiratory Tract InfectionsZyrene RiveraNo ratings yet
- Prepared By: Ulfat Amin MSC Pediatric NursingDocument25 pagesPrepared By: Ulfat Amin MSC Pediatric NursingAngelic khanNo ratings yet
- Laryngitis and PericarditisDocument17 pagesLaryngitis and Pericarditis2B-4- TUNAC, Avvy Charlotte R.No ratings yet
- Child With Respiratory DisorderDocument48 pagesChild With Respiratory DisorderEmjay JapitanaNo ratings yet
- Sinusitis DefinitionDocument7 pagesSinusitis Definitionfaye kimNo ratings yet
- Microbial Diseases of Respiratory SystemDocument27 pagesMicrobial Diseases of Respiratory SystemPermalino Borja Rose AnneNo ratings yet
- Respiratory System (Common Diseases)Document23 pagesRespiratory System (Common Diseases)Philip YansonNo ratings yet
- Bloodborne Pathogens TrainingDocument102 pagesBloodborne Pathogens Trainingapi-311432115No ratings yet
- Formularium Pertamina 2017 PDFDocument51 pagesFormularium Pertamina 2017 PDFyohanNo ratings yet
- TracheomalaciaDocument11 pagesTracheomalaciaAgung BhaktiyarNo ratings yet
- What Causes Pain Behind The KneeDocument7 pagesWhat Causes Pain Behind The KneeRatnaPrasadNalamNo ratings yet
- Li V Sps. SolimanDocument4 pagesLi V Sps. SolimanTriccie MangueraNo ratings yet
- ConstipationDocument11 pagesConstipationAsma SikanderNo ratings yet
- Hypnosis and Deep Relaxation in Static ApneaDocument16 pagesHypnosis and Deep Relaxation in Static ApneaMichael LeeNo ratings yet
- V2 Reimagine Reconstruction Ligament Brochure Digital 0322Document71 pagesV2 Reimagine Reconstruction Ligament Brochure Digital 0322Juan Martinez Del AngelNo ratings yet
- Danafarber CancerDocument273 pagesDanafarber CanceriulianamileaNo ratings yet
- Treatment and Prevention of Streptococcal Tonsillopharyngitis - UpToDateDocument14 pagesTreatment and Prevention of Streptococcal Tonsillopharyngitis - UpToDateJavier Manuel Escobedo CalderónNo ratings yet
- PDR Physicians Desk Reference 2016Document5 pagesPDR Physicians Desk Reference 2016Randy GroverNo ratings yet
- Faradic Aversion TherapyDocument4 pagesFaradic Aversion Therapyrichieerishi100% (1)
- ESPEN Guidelines On Nutritional Support For Polymorbid Internal Med PatDocument18 pagesESPEN Guidelines On Nutritional Support For Polymorbid Internal Med PatAmany SalamaNo ratings yet
- MPCB LimitsDocument6 pagesMPCB LimitsKunalGopalAgiwaleNo ratings yet
- Down SyndromeDocument18 pagesDown Syndromepreciouslacdan86% (7)
- Dry Needling Versus Acupuncture: The Ongoing Debate: Acupuncture in Medicine November 2015Document8 pagesDry Needling Versus Acupuncture: The Ongoing Debate: Acupuncture in Medicine November 2015ريما ميماNo ratings yet
- Otorhinolaryngology: Therapeutic Approach To Pediatric Acute Mastoiditis - An UpdateDocument9 pagesOtorhinolaryngology: Therapeutic Approach To Pediatric Acute Mastoiditis - An UpdateImelda LieNo ratings yet
- Assignment On IMNCIDocument3 pagesAssignment On IMNCIcharanjit kaurNo ratings yet
- Scabies Jurnal PDFDocument6 pagesScabies Jurnal PDFImam Hakim SuryonoNo ratings yet
- Ozone Application in Apple ProcessingDocument2 pagesOzone Application in Apple ProcessingCosimo RocheNo ratings yet
- Anaphylactic ShockDocument19 pagesAnaphylactic ShockrutiranNo ratings yet
- Christopher Shaw 1 SubstanceAbuse CriminalActivity PDFDocument51 pagesChristopher Shaw 1 SubstanceAbuse CriminalActivity PDFWKYC.comNo ratings yet
- ADR Cuff Pressure Gauges MonitorsDocument1 pageADR Cuff Pressure Gauges MonitorsssangssNo ratings yet
- Early SensoryDocument6 pagesEarly SensorySteven FlynnNo ratings yet
- A-PULMO - (LEE-TAN-CONSTANTINO) - Prelims (TD) B - Pulmo - (Lee-Tan-Constantino) - PrelimsDocument17 pagesA-PULMO - (LEE-TAN-CONSTANTINO) - Prelims (TD) B - Pulmo - (Lee-Tan-Constantino) - PrelimsJohn Paulo CatacutanNo ratings yet
- To, Ms. Sunayana Vikhe College of Pharmacy Pravara Nagar Dist. A' NagarDocument6 pagesTo, Ms. Sunayana Vikhe College of Pharmacy Pravara Nagar Dist. A' NagarSunayana VikheNo ratings yet
- TALK 1 - MR Benjamin Ho (Private Practice)Document6 pagesTALK 1 - MR Benjamin Ho (Private Practice)Annabel KohNo ratings yet
- Engagement in Child and Adolescent Treatment - The Role of Parental Cognitions and AttributionsDocument16 pagesEngagement in Child and Adolescent Treatment - The Role of Parental Cognitions and Attributionssolutions4familyNo ratings yet
- Genetics 2868Document8 pagesGenetics 2868Farrukh Ali KhanNo ratings yet
- Lymph Nodes and Lymphadenopathy in CancerDocument1 pageLymph Nodes and Lymphadenopathy in CancerEddy Lopez GuerreroNo ratings yet