You might also like
- Nursing Management & LeadershipDocument44 pagesNursing Management & Leadershipxr4dmNo ratings yet
- Health Care System Performance: By: Masheal Alsouhih Amjad Almutairi Supervised By: DR - Hanan AlgorashiDocument49 pagesHealth Care System Performance: By: Masheal Alsouhih Amjad Almutairi Supervised By: DR - Hanan AlgorashiAmjad100% (1)
- TQM Lec 1Document15 pagesTQM Lec 1Dina Lutfy SharafNo ratings yet
- Qid Model Plans ClinicsDocument16 pagesQid Model Plans Clinicsseshuv2No ratings yet
- 13 Patient Saefty and Quality ImprovementDocument36 pages13 Patient Saefty and Quality ImprovementShafiq Ur RahmanNo ratings yet
- Quality Assurence in Obstetrical and Gynaecological UnitDocument10 pagesQuality Assurence in Obstetrical and Gynaecological UnitVeena DalmeidaNo ratings yet
- Clinical GovernanceDocument9 pagesClinical GovernanceSajid Rahman100% (1)
- QPS Sample GuidelinesDocument23 pagesQPS Sample GuidelinesSafiqulatif AbdillahNo ratings yet
- Nursing Audit-Definition, History, Purposes, Methods, Characteristics, ProcessDocument3 pagesNursing Audit-Definition, History, Purposes, Methods, Characteristics, ProcessGladys YaresNo ratings yet
- 2.quality Assurance in NursingDocument7 pages2.quality Assurance in NursingNancy SamuelNo ratings yet
- Practice Standards For Obstetric and Gynaecological UnitDocument27 pagesPractice Standards For Obstetric and Gynaecological UnitRDi J100% (1)
- Quality in Health Care:: DefinitionDocument7 pagesQuality in Health Care:: DefinitionREVATHI H KNo ratings yet
- AUDITDocument6 pagesAUDITJay RathvaNo ratings yet
- Value Health Care Quality in Other FieldsDocument16 pagesValue Health Care Quality in Other Fieldshemant kumarNo ratings yet
- Nursing AuditDocument16 pagesNursing AuditAnusha VergheseNo ratings yet
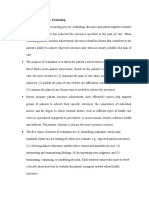
- Key Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthDocument4 pagesKey Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthmsbunnileeNo ratings yet
- Quality Assurance (Autosaved)Document75 pagesQuality Assurance (Autosaved)OGU CourageNo ratings yet
- IntroductionDocument7 pagesIntroductionMadhu Bishnoi100% (1)
- Nursing AuditDocument60 pagesNursing AuditValliammalShanmugam100% (8)
- Risk Management PDFDocument20 pagesRisk Management PDFNikhil ShahaneNo ratings yet
- Quality Assurance in NursingDocument8 pagesQuality Assurance in NursingAnusha VergheseNo ratings yet
- Nursing AuditDocument26 pagesNursing AuditJoe ShewaleNo ratings yet
- Qulity AssurancesDocument11 pagesQulity Assurancessteffy christNo ratings yet
- ControllingDocument8 pagesControllingSheilaMacatangayNo ratings yet
- Nursing AuditDocument6 pagesNursing Auditpak huda100% (1)
- Quality-Improvement PlanDocument11 pagesQuality-Improvement Planyhm70071No ratings yet
- STAN5 JCI AccreditationDocument57 pagesSTAN5 JCI AccreditationYulinur FirdausNo ratings yet
- Nursing AuditDocument21 pagesNursing AuditSam TullyNo ratings yet
- Health Care Quality ConceptsDocument11 pagesHealth Care Quality Conceptsmike700usNo ratings yet
- Clinical Pathways and Nurses.Document3 pagesClinical Pathways and Nurses.Natukunda Dianah100% (1)
- Clinical GovernanceDocument4 pagesClinical GovernanceGayani UdayangaNo ratings yet
- Critical Pathway: Clinical Pathways Have Four Main Components (Hill, 1994, Hill 1998)Document5 pagesCritical Pathway: Clinical Pathways Have Four Main Components (Hill, 1994, Hill 1998)pooja singhNo ratings yet
- Final Qa PDFDocument24 pagesFinal Qa PDFRenita ChrisNo ratings yet
- Audit As A Quality Control Tool ReportDocument30 pagesAudit As A Quality Control Tool ReportJenno Ray Senal67% (3)
- 2nd SEMDocument3 pages2nd SEMMj Kenneth IlayaNo ratings yet
- Quality Assurance in Perioperative NursingDocument39 pagesQuality Assurance in Perioperative NursingbummyNo ratings yet
- Integrasi Manajemen Risiko, Keselamatan Pasien Dan Manajemen MutuDocument32 pagesIntegrasi Manajemen Risiko, Keselamatan Pasien Dan Manajemen Mutubrigitta_bikaNo ratings yet
- Nursing AuditDocument22 pagesNursing AuditBinal Joshi100% (3)
- Clin MNGR IIIDocument54 pagesClin MNGR IIIbaskorosanjayaNo ratings yet
- AN Assignment On Nursing Audit SUBJECT: Nursing ManagementDocument6 pagesAN Assignment On Nursing Audit SUBJECT: Nursing ManagementMansi Dabola100% (1)
- QUALITY ProgrammeDocument9 pagesQUALITY ProgrammeYadu HariNo ratings yet
- Ateneo de Davao University Graduate SchoolDocument4 pagesAteneo de Davao University Graduate SchoolDennis Nabor Muñoz, RN,RMNo ratings yet
- Quality AssuranceDocument57 pagesQuality AssuranceAmy Lalringhluani67% (3)
- Self EvaluationDocument4 pagesSelf EvaluationSonu Singh100% (2)
- Principles of Management: Neeraj Lal - Vice President (Quality & Strategic Alliances) Shalby HospitalsDocument39 pagesPrinciples of Management: Neeraj Lal - Vice President (Quality & Strategic Alliances) Shalby HospitalsDr. Rakshit SolankiNo ratings yet
- Nursingprocess Assessing 111105015609 Phpapp01Document71 pagesNursingprocess Assessing 111105015609 Phpapp01ALmik HussinNo ratings yet
- Clinical Audit For Medical StudentsDocument6 pagesClinical Audit For Medical StudentsAmal SaeedNo ratings yet
- Clinical GovernanceDocument25 pagesClinical Governancesantosaerwin6591100% (1)
- IQIPS Standard v2, 2020Document20 pagesIQIPS Standard v2, 2020TharshiniNo ratings yet
- Service & Quality, Management in Hospitals (S&QMH) : Subject Code: CC2110 Roll No: MHA19102Document26 pagesService & Quality, Management in Hospitals (S&QMH) : Subject Code: CC2110 Roll No: MHA19102Dr. Ebinesh AntonyNo ratings yet
- Quality Assurance in NursingDocument7 pagesQuality Assurance in Nursingchaithanya100% (1)
- Quality Assurance ProcessDocument3 pagesQuality Assurance ProcessJane ChinonsoNo ratings yet
- Total Quality Management in Health Care Total Quality Management in Health CareDocument23 pagesTotal Quality Management in Health Care Total Quality Management in Health CareFaisal AlzhraniNo ratings yet
- ControllingDocument8 pagesControllingAnjo Pasiolco Canicosa100% (2)
- Hello Good MorningDocument5 pagesHello Good MorningAllan SaquinNo ratings yet
- Patient Safety PlanDocument4 pagesPatient Safety PlanDhananjay SainiNo ratings yet
- 9.4.20 An - NF - Unit 5Document52 pages9.4.20 An - NF - Unit 5lisafelixNo ratings yet
- Nursing AuditDocument6 pagesNursing AuditAnusha VergheseNo ratings yet
- Introduction to Clinical Effectiveness and Audit in HealthcareFrom EverandIntroduction to Clinical Effectiveness and Audit in HealthcareNo ratings yet
- Medical Records ManagementDocument52 pagesMedical Records ManagementMulat AlemuNo ratings yet
- Nursing and Midwifery Care ServicesDocument40 pagesNursing and Midwifery Care ServicesMulat AlemuNo ratings yet
- Medical Equipment Management PresentationDocument34 pagesMedical Equipment Management PresentationMulat AlemuNo ratings yet
- Federal - Teachning Hospitals ManagementDocument27 pagesFederal - Teachning Hospitals ManagementMulat AlemuNo ratings yet
- Outpatient ServiceDocument28 pagesOutpatient ServiceMulat AlemuNo ratings yet
- Health Financing and Asset ManagementDocument51 pagesHealth Financing and Asset ManagementMulat AlemuNo ratings yet
- Liaison, Referral and Social ServicesDocument25 pagesLiaison, Referral and Social ServicesMulat AlemuNo ratings yet
- Maternal, Neonatal and Child Health ServicesDocument49 pagesMaternal, Neonatal and Child Health ServicesGebre GutetaNo ratings yet
- Inpatient ServiceDocument34 pagesInpatient ServiceGebre GutetaNo ratings yet
- Laboratory ServicesDocument43 pagesLaboratory ServicesMulat AlemuNo ratings yet
- Infection Prevention and Patient SafetyDocument35 pagesInfection Prevention and Patient SafetyMulat AlemuNo ratings yet
- Hospital Leadership, Management and GovernanceDocument46 pagesHospital Leadership, Management and GovernanceGebre GutetaNo ratings yet
- Monitoring and ReportingDocument21 pagesMonitoring and ReportingMulat AlemuNo ratings yet
- Developing and Implementing A Monitoring & Evaluation Plan: DraftDocument32 pagesDeveloping and Implementing A Monitoring & Evaluation Plan: DraftRuby GarciaNo ratings yet
- Developing Creative Leadership in A Public Service OrganisationDocument11 pagesDeveloping Creative Leadership in A Public Service OrganisationAzim MohammedNo ratings yet
- Barriers in Constrction ManagementDocument47 pagesBarriers in Constrction Managementhimadri.banerji60No ratings yet
- Enter Gov N Enterprie Engineering - 2009 (Additional)Document445 pagesEnter Gov N Enterprie Engineering - 2009 (Additional)suryapribadiNo ratings yet
- BSCADocument20 pagesBSCAROOMA SALEEMNo ratings yet
- Human Capital A Source of Competitive Advantage "Ideas For Strategic Leadership"Document8 pagesHuman Capital A Source of Competitive Advantage "Ideas For Strategic Leadership"muna moonoNo ratings yet
- HRM As-2 Bilal Masood, 28858Document15 pagesHRM As-2 Bilal Masood, 28858Muzzamil JanjuaNo ratings yet
- Market Need Analysis Define The Market Need For The New BusinessDocument2 pagesMarket Need Analysis Define The Market Need For The New BusinessCarmela De Juan100% (3)
- Metrolab Industries V ConfesorDocument10 pagesMetrolab Industries V ConfesorbrendamanganaanNo ratings yet
- Why Australia?: Student Interview Questionnaire For AustraliaDocument7 pagesWhy Australia?: Student Interview Questionnaire For AustraliaAnonymous oryqjfYONo ratings yet
- EDE Practical 1Document4 pagesEDE Practical 1Rugved BhalekarNo ratings yet
- BMPD AssignmentsDocument4 pagesBMPD Assignmentsjd2saiNo ratings yet
- MRP Vs MPSDocument3 pagesMRP Vs MPSmeddebyounesNo ratings yet
- NRB Syllabus PDFDocument4 pagesNRB Syllabus PDFnavbhusal100% (11)
- POM Module 2 StudentDocument5 pagesPOM Module 2 Studentjeliannediaz785No ratings yet
- PTC 2019 BrochureDocument24 pagesPTC 2019 BrochurePhD to Consulting ConferenceNo ratings yet
- 2021 Exam-Nov-2021-Exam-PaperDocument8 pages2021 Exam-Nov-2021-Exam-Paperkellz accountingNo ratings yet
- Pre-Planning and PlanningDocument9 pagesPre-Planning and PlanningJanellaReanoReyesNo ratings yet
- HRM Sector in Bangladesh Problem & ProspectDocument27 pagesHRM Sector in Bangladesh Problem & Prospectস্ট্রোম ব্রেকার80% (5)
- All About AvanadeDocument16 pagesAll About AvanadeSunil PatidarNo ratings yet
- Introduction To Hotel IndustryDocument14 pagesIntroduction To Hotel IndustryImrul StudioNo ratings yet
- Module On PESTLE AnalysisDocument8 pagesModule On PESTLE AnalysisSunshine NavuisoNo ratings yet
- CRM Unit - 3Document26 pagesCRM Unit - 3jayNo ratings yet
- Assignment On Corporate ReportingDocument6 pagesAssignment On Corporate ReportingMusic & ArtNo ratings yet
- Adam Bataineh Ch5Document10 pagesAdam Bataineh Ch5Omar AssafNo ratings yet
- Module 1.2 - Strategic Management ProcessDocument4 pagesModule 1.2 - Strategic Management Processnemuel BarbaNo ratings yet
- WarehousingDocument33 pagesWarehousingMervyn Joe Sebastian100% (2)
- BI Developer - Job DescriptionDocument2 pagesBI Developer - Job DescriptionSolomon Cosmin IonutNo ratings yet
- Six Sigma PresentationDocument17 pagesSix Sigma PresentationDhular HassanNo ratings yet
- TQ For 1st Quarter Org and MGNT 11Document2 pagesTQ For 1st Quarter Org and MGNT 11Kee Jay PondocNo ratings yet