0% found this document useful (0 votes)
81 views30 pagesAtelectasis and Pneumothorax Overview
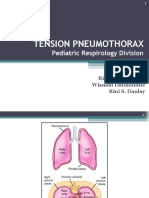
The document discusses atelectasis and pneumothorax. It defines atelectasis as a partial or complete collapse of the lungs and describes different types including obstructive and non-obstructive. It also defines pneumothorax as air in the pleural cavity and describes different types. Treatment options are discussed including re-expanding the lungs through drainage of fluid or air and clearing obstructions.
Uploaded by
ashoaib0313Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PPT, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
81 views30 pagesAtelectasis and Pneumothorax Overview
The document discusses atelectasis and pneumothorax. It defines atelectasis as a partial or complete collapse of the lungs and describes different types including obstructive and non-obstructive. It also defines pneumothorax as air in the pleural cavity and describes different types. Treatment options are discussed including re-expanding the lungs through drainage of fluid or air and clearing obstructions.
Uploaded by
ashoaib0313Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PPT, PDF, TXT or read online on Scribd