You might also like
- Succubus EvocationDocument246 pagesSuccubus Evocationlmsanthosh kumar87% (15)
- Papyri Graecae MagicaeDocument210 pagesPapyri Graecae Magicaemyuri ayaka100% (13)
- TOEIC Revision OverviewDocument1 pageTOEIC Revision Overviewreadup1No ratings yet
- Epidemiology ReviewDocument10 pagesEpidemiology ReviewSaurabhNo ratings yet
- Bias in EpidemiologyDocument5 pagesBias in EpidemiologyEga JayaNo ratings yet
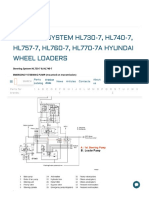
- Steering System HL730-7, HL740-7, HL757-7, HL760-7, HL770-7A Hyundai Wheel Loaders - Industry Articles - in Online Store BuyAftermarketPartsDocument25 pagesSteering System HL730-7, HL740-7, HL757-7, HL760-7, HL770-7A Hyundai Wheel Loaders - Industry Articles - in Online Store BuyAftermarketPartsKarthikVijayNo ratings yet
- ASSESSMENT OF Periodontal Risk Factors and IndicatorsDocument113 pagesASSESSMENT OF Periodontal Risk Factors and IndicatorsNeal TorwaneNo ratings yet
- Association and CausationDocument111 pagesAssociation and CausationKshitij ChaurasiaNo ratings yet
- BIAS. Confounding and Effect ModificationDocument10 pagesBIAS. Confounding and Effect ModificationCSilva16No ratings yet
- BWW 2012 New Tool List INDIA MarketDocument4 pagesBWW 2012 New Tool List INDIA Marketcricketabhi100% (1)
- Methods Used in EpidemologyDocument53 pagesMethods Used in EpidemologySameera banuNo ratings yet
- Epidemiology: Dr. Siswanto, M.SCDocument66 pagesEpidemiology: Dr. Siswanto, M.SCArinTa TyArlieNo ratings yet
- EpidemiologyDocument40 pagesEpidemiologyCharityOchiengNo ratings yet
- Cross Sectional Study in EpidemiologyDocument10 pagesCross Sectional Study in EpidemiologyInes GumayyNo ratings yet
- 812 Ancient IndiaDocument49 pages812 Ancient IndiaJahnavi SinghNo ratings yet
- Rights and Duties of Buyer and SellerDocument5 pagesRights and Duties of Buyer and Sellerselvaa kumarNo ratings yet
- Association & CausationDocument23 pagesAssociation & CausationRahul NetragaonkarNo ratings yet
- Causation in EpidemiologyDocument3 pagesCausation in Epidemiologypuskesmas beloNo ratings yet
- Sesi 3C - Konsep Penyebab Penyakit IiDocument100 pagesSesi 3C - Konsep Penyebab Penyakit IidewiNo ratings yet
- Web of CausationDocument39 pagesWeb of CausationAhmedStatisticsNo ratings yet
- Association and CausationDocument60 pagesAssociation and Causationsehar_bashirNo ratings yet
- CausalityDocument3 pagesCausalityJoachim “Jayrz” MwambireNo ratings yet
- Web of Causation Exposure and Disease Outcomes: Thomas Songer, PHDDocument35 pagesWeb of Causation Exposure and Disease Outcomes: Thomas Songer, PHDAbuzar AliNo ratings yet
- Association and CausationDocument16 pagesAssociation and CausationnyangaraNo ratings yet
- 5association and Causation - Pptx.docx (FDocument7 pages5association and Causation - Pptx.docx (Falhashemisaqr100% (1)
- 3 - Causal - Inference - in - EpidemiologyDocument63 pages3 - Causal - Inference - in - Epidemiologyfareehakanwar93No ratings yet
- Analytical Epidemiology: Dr. Eman Khammas Al-Sadi Chief of Community DepartmentDocument23 pagesAnalytical Epidemiology: Dr. Eman Khammas Al-Sadi Chief of Community DepartmentEman KhammasNo ratings yet
- Case ControlDocument45 pagesCase ControlIsmail QamarNo ratings yet
- Epidemiology Concept of CauseDocument45 pagesEpidemiology Concept of CauseAiszel Angeli Pepito LigoNo ratings yet
- Association & Causation 6Document13 pagesAssociation & Causation 6Mongolian MutuNo ratings yet
- Hills Criteria of Causation - ZiaDocument16 pagesHills Criteria of Causation - ZiaAli FrhdNo ratings yet
- Cause and Effect Relationship - PPTX Latest BinaDocument37 pagesCause and Effect Relationship - PPTX Latest BinaHaalaNo ratings yet
- Community - 07Document4 pagesCommunity - 07Mohammad AlrefaiNo ratings yet
- Disease Causation 2Document32 pagesDisease Causation 2andualem werkinehNo ratings yet
- Theory of CausalityDocument18 pagesTheory of CausalityMazayazka Zahiya ShofiNo ratings yet
- Nested Case Control StudyDocument6 pagesNested Case Control StudyFarah FarahNo ratings yet
- CausationDocument22 pagesCausationdrdewimsNo ratings yet
- Risk Factors Underlying Disasters: Climate ChangeDocument8 pagesRisk Factors Underlying Disasters: Climate ChangeAdriane GarciaNo ratings yet
- Lesson 4Document59 pagesLesson 4chiyumbabeatriceNo ratings yet
- Causal Inference in Cancer EpidemiologyDocument22 pagesCausal Inference in Cancer EpidemiologyATHUMANI JUMBENo ratings yet
- Causal I DadDocument41 pagesCausal I DadYover Lucero CuevaNo ratings yet
- EpidemiologyDocument18 pagesEpidemiologyRose Jean C. OtodNo ratings yet
- Causal Inferences in Epidemiological Studies 2022Document41 pagesCausal Inferences in Epidemiological Studies 2022Kanwal KhanNo ratings yet
- Analysis of Cause Effect RelationshipDocument50 pagesAnalysis of Cause Effect RelationshipRida AwwalNo ratings yet
- Measuring of Association in EpidemiologyDocument21 pagesMeasuring of Association in EpidemiologyMazayazka Zahiya ShofiNo ratings yet
- Epidemiology (Approaches &methods), Disease Causation and ScreeningDocument37 pagesEpidemiology (Approaches &methods), Disease Causation and ScreeningSyed Arifa AndrabiNo ratings yet
- Epi Descriptive Study DesignsDocument4 pagesEpi Descriptive Study DesignsAndrea BardalesNo ratings yet
- Clinical Types of Epidemiological StudiesDocument3 pagesClinical Types of Epidemiological StudiesEduardo Proaño100% (1)
- Epi Controlling For ConfoundingDocument4 pagesEpi Controlling For ConfoundingcharlesNo ratings yet
- Causation Concept: Principles of EpidemiologyDocument28 pagesCausation Concept: Principles of EpidemiologyvhiiaNo ratings yet
- 11 Concept of CauseDocument32 pages11 Concept of CausemwambungupNo ratings yet
- Konsep KausalitasDocument29 pagesKonsep Kausalitasbianca bungaNo ratings yet
- Causes RothmanDocument6 pagesCauses RothmanSamuel Andrés AriasNo ratings yet
- DR - Abdulfatah Hamarahm HawrameiDocument44 pagesDR - Abdulfatah Hamarahm HawrameiRagash H. MohammedNo ratings yet
- DR Ashwin Raj K K Assistant Professor Department of Community Medicine Mes Medical College PerinthalmannaDocument50 pagesDR Ashwin Raj K K Assistant Professor Department of Community Medicine Mes Medical College PerinthalmannaAshwinRajNo ratings yet
- Chance, Bias, ConfoundingDocument33 pagesChance, Bias, ConfoundingseoukieNo ratings yet
- Epi DefinitionsDocument3 pagesEpi DefinitionsTim GibbsNo ratings yet
- Sec A Confounding and VariabilityDocument15 pagesSec A Confounding and VariabilityLabiba TasnimNo ratings yet
- Epi L3 For Pharmacy Dep..Document19 pagesEpi L3 For Pharmacy Dep..SoromeNo ratings yet
- EpidemiologyDocument66 pagesEpidemiologyTooba NaeemNo ratings yet
- Concept of Risk Factor - NCDEDocument9 pagesConcept of Risk Factor - NCDEFirly Azra GhassanieNo ratings yet
- Correlation and Causation WorksheetDocument4 pagesCorrelation and Causation WorksheeteonsNo ratings yet
- Lecture Notes On Epidemiological Studies For UndergraduatesDocument41 pagesLecture Notes On Epidemiological Studies For UndergraduatespopasorinemilianNo ratings yet
- Premed - SPH - 2022Document55 pagesPremed - SPH - 2022Tofik MohammedNo ratings yet
- Confounding TranslateDocument19 pagesConfounding TranslateJonesius Eden ManoppoNo ratings yet
- Multicausality: Effect ModificationDocument33 pagesMulticausality: Effect ModificationDani Yitu MedanituNo ratings yet
- Community As Partner - Chapter 3Document4 pagesCommunity As Partner - Chapter 3KTNo ratings yet
- Experimental EpidemiologyDocument17 pagesExperimental EpidemiologyDr Sumit KarNo ratings yet
- Epidemiological StudiesDocument25 pagesEpidemiological StudiesDr Sumit KarNo ratings yet
- Screening TestDocument28 pagesScreening TestDr Sumit KarNo ratings yet
- Dynamics of Disease TransmissionDocument24 pagesDynamics of Disease TransmissionDr Sumit KarNo ratings yet
- Bsi 29 JulDocument12 pagesBsi 29 JulDr Sumit KarNo ratings yet
- Retained Tensile Strength TestDocument6 pagesRetained Tensile Strength TestVikas ThakarNo ratings yet
- Catalog EGR VOL-StahlDocument9 pagesCatalog EGR VOL-StahlTetroVorinNo ratings yet
- Computer Aided InstructionDocument22 pagesComputer Aided InstructionIsrael Anthony AlmascoNo ratings yet
- CFT-Technical Analysis CompressedDocument1 pageCFT-Technical Analysis CompressedGlenden KhewNo ratings yet
- Dissertation On Environmental Law in IndiaDocument8 pagesDissertation On Environmental Law in IndiaWriteMyPaperInApaFormatSingapore100% (1)
- Template 02Document1 pageTemplate 02deivy erazoNo ratings yet
- Using The Netkey Utility For Managing Csi Network LicensesDocument7 pagesUsing The Netkey Utility For Managing Csi Network Licensesthanzawtun1981No ratings yet
- What Internat IsDocument3 pagesWhat Internat Isdewa cuanajaNo ratings yet
- Question-02 Human Resource ManagementDocument4 pagesQuestion-02 Human Resource ManagementRiya SinghNo ratings yet
- Instructions To Bidders: Rehabilitation of 50kW Solar Wind Hybrid Power Plant in Compliance With PPRA RULES, 2014Document12 pagesInstructions To Bidders: Rehabilitation of 50kW Solar Wind Hybrid Power Plant in Compliance With PPRA RULES, 2014Dipak BayalkotiNo ratings yet
- Ns Unit 3Document36 pagesNs Unit 3sharath_rakkiNo ratings yet
- In Uence of Type of Loading (Tension or Bending) On Cracking Behaviour of Reinforced Concrete Elements. Experimental StudyDocument26 pagesIn Uence of Type of Loading (Tension or Bending) On Cracking Behaviour of Reinforced Concrete Elements. Experimental Studydmt7nzztcmNo ratings yet
- Electrical Engineering FundamentalsDocument3 pagesElectrical Engineering FundamentalsDontNo ratings yet
- Industry and Market AnalysisDocument8 pagesIndustry and Market AnalysisAkhil SoniNo ratings yet
- Mathematics of in V 004275 MBPDocument584 pagesMathematics of in V 004275 MBPEian chin mana-ayNo ratings yet
- AgroBoga 050923 (2po)Document2 pagesAgroBoga 050923 (2po)AGRO BOGA UTAMANo ratings yet
- Business Studies Project - BHARAT BHARATDocument11 pagesBusiness Studies Project - BHARAT BHARATabarajitha sureshkumarNo ratings yet
- GEC 105 Purposive Communication Module 3Document27 pagesGEC 105 Purposive Communication Module 3Jenedee UniformeNo ratings yet
- ScoutsDocument284 pagesScoutsJoMarie130% (1)
- CNC Programming: Profile No.: 272 NIC Code:62011Document10 pagesCNC Programming: Profile No.: 272 NIC Code:62011Sanyam BugateNo ratings yet
- School Consolidated Report On MPS: Puting Buhangin Elementary SchoolDocument14 pagesSchool Consolidated Report On MPS: Puting Buhangin Elementary SchoolVince Michael YtangNo ratings yet
- LexicographyDocument4 pagesLexicographyKoko channelNo ratings yet