You might also like
- 2 TSHDocument7 pages2 TSHNashat SaadiNo ratings yet
- Nilanjan Bhowmick, Cology-11Document10 pagesNilanjan Bhowmick, Cology-11Nilanjan BhowmickNo ratings yet
- Thyroid Diet : Thyroid Solution Diet & Natural Treatment Book For Thyroid Problems & Hypothyroidism Revealed!From EverandThyroid Diet : Thyroid Solution Diet & Natural Treatment Book For Thyroid Problems & Hypothyroidism Revealed!Rating: 1 out of 5 stars1/5 (1)
- Endocrine SystemDocument30 pagesEndocrine SystemAkshat RastogiNo ratings yet
- Debjani Ghosh 99Document10 pagesDebjani Ghosh 99Nilanjan BhowmickNo ratings yet
- ENDOCRINE SYSTEM DISORDERS Unit 1Document8 pagesENDOCRINE SYSTEM DISORDERS Unit 1Rizza Mae MaglacionNo ratings yet
- Endocrine Physiology Lecture by Mrs M MUTSANGU POLY ND1Document56 pagesEndocrine Physiology Lecture by Mrs M MUTSANGU POLY ND1letwinemwale02No ratings yet
- Thyroid Health: The Thyroid Solution Diet ExposedFrom EverandThyroid Health: The Thyroid Solution Diet ExposedRating: 3 out of 5 stars3/5 (2)
- Endocrine System ProvidedDocument73 pagesEndocrine System Providedummezainhumayra11No ratings yet
- Endo Lect 7-THDocument30 pagesEndo Lect 7-THdoctorrfarrukhNo ratings yet
- 2.0 HormonesDocument5 pages2.0 HormonesHry WkNo ratings yet
- Chemical Coordination and Integration by - Dr. Sunita SaxenaDocument66 pagesChemical Coordination and Integration by - Dr. Sunita SaxenaDivya AgarawalNo ratings yet
- Functional Anatomy and PhysiologyDocument38 pagesFunctional Anatomy and PhysiologyNawalNo ratings yet
- Thyroid Gland 1Document16 pagesThyroid Gland 1Minal JadhavNo ratings yet
- HomeostasisDocument51 pagesHomeostasisKarla HyltonNo ratings yet
- Endocrine System AnatomyDocument41 pagesEndocrine System Anatomypizzyray640No ratings yet
- Module 22 HormonesDocument23 pagesModule 22 HormonesCrystal ManguneNo ratings yet
- Farmacoendocrino 2008Document58 pagesFarmacoendocrino 2008Eduardo ValdezNo ratings yet
- Part 3 - MEDTERM-117 LECDocument6 pagesPart 3 - MEDTERM-117 LECfrechel kimNo ratings yet
- Thyroid DisordersNewDocument47 pagesThyroid DisordersNewTri Octavia SitorusNo ratings yet
- Anatomy and Physiology Chapter 21 The Sensory SystemDocument34 pagesAnatomy and Physiology Chapter 21 The Sensory SystemThanh Nguyen VanNo ratings yet
- Chemical Co - OrdinationDocument21 pagesChemical Co - OrdinationManinder KaurNo ratings yet
- Endocrine System and Excretion WordDocument10 pagesEndocrine System and Excretion WordJoachim “Jayrz” MwambireNo ratings yet
- CombinedDocument40 pagesCombinedshortsmotivation87No ratings yet
- Endocrine System 13 معدلDocument11 pagesEndocrine System 13 معدلhanaalhadidi567No ratings yet
- Assessment and Management of Patients With Endocrine DisordersDocument11 pagesAssessment and Management of Patients With Endocrine DisordersLesley GonzalezNo ratings yet
- Endocrine System 2Document50 pagesEndocrine System 2park jongseongNo ratings yet
- Thyroid and Antithyroid DrugsDocument59 pagesThyroid and Antithyroid DrugsKhairunnisa LoqmanNo ratings yet
- Thyroid HormonesDocument7 pagesThyroid HormonesAbdullah EssaNo ratings yet
- Assessment and Management of Patients With Endocrine DisordersDocument46 pagesAssessment and Management of Patients With Endocrine Disordersamal100% (1)
- Hormones - Thyroid Axis: Sujin Bao, PH.DDocument29 pagesHormones - Thyroid Axis: Sujin Bao, PH.DLunaLureNo ratings yet
- The Endocrine System Overview/ Introduction: Nur112: Anatomy and Physiology ISU Echague - College of NursingDocument6 pagesThe Endocrine System Overview/ Introduction: Nur112: Anatomy and Physiology ISU Echague - College of NursingWai KikiNo ratings yet
- Endocrine System/socialDocument33 pagesEndocrine System/socialrpant3165No ratings yet
- Hyperthyroid 170715182805Document71 pagesHyperthyroid 170715182805Suryati HusinNo ratings yet
- Hormones: Prof. Dr. V P SoniDocument21 pagesHormones: Prof. Dr. V P SoniPadma VishwanathNo ratings yet
- Thyroid HormonesDocument47 pagesThyroid Hormonesamalia100% (1)
- 77 - Thyroid Metabolic HormonesDocument6 pages77 - Thyroid Metabolic Hormonesmanjitashet4049No ratings yet
- Pharmacology of The Endocrine SystemDocument74 pagesPharmacology of The Endocrine SystemarpanabiswassshetyeNo ratings yet
- Production, Regulation, and Action of Thyroid HormonesDocument34 pagesProduction, Regulation, and Action of Thyroid HormonesStefanie Pramudita JayaNo ratings yet
- Corticotropins and GonadotropinsDocument39 pagesCorticotropins and GonadotropinsSudhakar LakavathNo ratings yet
- BioDocument9 pagesBioaatishsubash9b35832No ratings yet
- Endocrine Test 8 NotesDocument9 pagesEndocrine Test 8 NotesHayden ShulerNo ratings yet
- Physiology 1STDocument10 pagesPhysiology 1STGW LEGENDNo ratings yet
- 3.thyroid Hormones and DisordersDocument46 pages3.thyroid Hormones and DisorderssinayupeNo ratings yet
- Thyroid Hormones: Sherwin B. Toriano, RMT, MSMTDocument33 pagesThyroid Hormones: Sherwin B. Toriano, RMT, MSMTBenedikt WeinholdNo ratings yet
- Endocrine SystemDocument43 pagesEndocrine SystemJeanette RiosNo ratings yet
- Endocrine System: Pituitary Gland and HypothalamusDocument9 pagesEndocrine System: Pituitary Gland and HypothalamusRohan Sahu0% (1)
- HealthDocument59 pagesHealthAngesh PokharelNo ratings yet
- Lecture 4 Thyroid GlandsDocument41 pagesLecture 4 Thyroid GlandsBJ BermasNo ratings yet
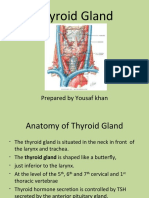
- Thyroid Gland: Prepared by Yousaf KhanDocument22 pagesThyroid Gland: Prepared by Yousaf KhanSalman KhanNo ratings yet
- Pharmacology of The Endocrine System PDFDocument74 pagesPharmacology of The Endocrine System PDFGlenn Perez71% (7)
- The Endocrine System: Presented By, MD Nasir Uddin Mahmood, Product Executive, Opsonin Pharma LimitedDocument24 pagesThe Endocrine System: Presented By, MD Nasir Uddin Mahmood, Product Executive, Opsonin Pharma LimitedMd Nasir Uddin Mahmood100% (2)
- Thyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!From EverandThyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!No ratings yet
- Endrocrine SystemDocument6 pagesEndrocrine SystemAsif Hasan NiloyNo ratings yet
- Endocrine SystemDocument24 pagesEndocrine Systempromisefo65No ratings yet
- Thyroid Anti Thyroid DrugsDocument25 pagesThyroid Anti Thyroid DrugsGunjan KalyaniNo ratings yet
- Metabolic Endocrinology (Week-2)Document8 pagesMetabolic Endocrinology (Week-2)wasimsafdarNo ratings yet
- Thyroid Gland PDFDocument47 pagesThyroid Gland PDFMACON824No ratings yet
- SAQ 2nd Week (Thyroid Gland)Document15 pagesSAQ 2nd Week (Thyroid Gland)Josephine BediakoNo ratings yet
- Name# Khursheed Ali Reg No# 17-ARID-6126Document15 pagesName# Khursheed Ali Reg No# 17-ARID-6126shahzeb bilalNo ratings yet
- Endocrine EmergenciesDocument33 pagesEndocrine EmergenciesbetyahNo ratings yet
- Armour Thyroid (Thyroid Tablets, USP) RX Only: I I NHDocument10 pagesArmour Thyroid (Thyroid Tablets, USP) RX Only: I I NHAdam GolsbyNo ratings yet
- HormonesDocument64 pagesHormonesNiyaz ShahriarNo ratings yet
- Semis 2 - Drugs Acting On The Endocrine System 2Document11 pagesSemis 2 - Drugs Acting On The Endocrine System 2Amiel Francisco Reyes100% (1)
- Optimizing Thyroid MedicationsDocument83 pagesOptimizing Thyroid MedicationsRicardo NovaisNo ratings yet
- HipothiroidDocument27 pagesHipothiroidYuji AdityaNo ratings yet
- 2013 ENDOCRINE PHARMACOLOGY Word Notes PDFDocument52 pages2013 ENDOCRINE PHARMACOLOGY Word Notes PDFNicole Opao100% (4)
- Thyroflex 4G Instruction Manual: Table of ContentDocument43 pagesThyroflex 4G Instruction Manual: Table of ContentLee LeeNo ratings yet
- Etiology-Hypothyroidism: Chronic Autoimmune ThyroiditisDocument4 pagesEtiology-Hypothyroidism: Chronic Autoimmune ThyroiditisNungky KusumaNo ratings yet
- Pharmacology Block 4Document83 pagesPharmacology Block 4Diwakesh C BNo ratings yet
- HHS Public Access: HypothyroidismDocument27 pagesHHS Public Access: HypothyroidismBrama AtmajaNo ratings yet
- Endocrine NursingDocument8 pagesEndocrine NursingBunny Bonny100% (5)
- Pharma 12Document16 pagesPharma 12Mary Roan RonatoNo ratings yet
- Pharmacology 2 NotesDocument21 pagesPharmacology 2 Notesgnikap_deleonNo ratings yet
- MCQ in Pharmacology New CuttedDocument14 pagesMCQ in Pharmacology New Cuttedhamid100% (1)
- Progesterone in Orthomolecular MedicineDocument68 pagesProgesterone in Orthomolecular Medicineederbernadino92No ratings yet
- Drugs Affecting The Body System - Endocrine SystemDocument69 pagesDrugs Affecting The Body System - Endocrine SystemFaye JavierNo ratings yet
- Weekly TipsDocument69 pagesWeekly TipsSharynn Kew Moore100% (1)
- Endocrine McQs 430Document41 pagesEndocrine McQs 430MalikQamarAbbasThaheem83% (6)
- Sustained Release T3 TherapyDocument10 pagesSustained Release T3 TherapyKARISHMA SHAIKHNo ratings yet
- RT3 ProblemDocument11 pagesRT3 Problemnatask100% (1)
- Drugs Acting On The Endocrine SystemDocument90 pagesDrugs Acting On The Endocrine SystemKATHERINE GRACE JOSENo ratings yet
- Propylthiouracil 2Document14 pagesPropylthiouracil 2Magdy Ali ELsherbenyNo ratings yet
- Polly Hattemer Book 4 HormonesDocument80 pagesPolly Hattemer Book 4 Hormonessusilorini100% (2)
- Journal of Internal Medicine - 2021 - Ross - Treating Hypothyroidism Is Not Always Easy When To Treat SubclinicalDocument13 pagesJournal of Internal Medicine - 2021 - Ross - Treating Hypothyroidism Is Not Always Easy When To Treat SubclinicalNAYSHA YANET CHAVEZ RONDINELNo ratings yet
- Breakthrough Discovery - Need For T3 Could Be Genetic DR Gary PepperDocument4 pagesBreakthrough Discovery - Need For T3 Could Be Genetic DR Gary PepperAna SmithNo ratings yet
- Phamacology Set 2: Page 1 of 24Document24 pagesPhamacology Set 2: Page 1 of 24Jonille EchevarriaNo ratings yet
- The Fat-Burner HandbookDocument143 pagesThe Fat-Burner HandbookNguyễn Bảo Minh75% (4)
- Heart Failure and Stroke Risks in Users of Liothyronine + LT4 Vs Lt4 Alone 2022Document8 pagesHeart Failure and Stroke Risks in Users of Liothyronine + LT4 Vs Lt4 Alone 2022NAYSHA YANET CHAVEZ RONDINELNo ratings yet
- 2021 The Enigma of Persistent Symptoms in Hypothyroid PatientsDocument8 pages2021 The Enigma of Persistent Symptoms in Hypothyroid PatientsPeter Albeiro Falla CortesNo ratings yet